Xolair Patient Enrollment Form
Xolair Patient Enrollment Form - The bias introduced by allowing enrollment of patients previously exposed to. Review the dosing schedule and your administration options. Web this service offers coverage support, patient assistance, and other useful information. For patients prescribed prxolair® for moderate to severe allergic asthma (aa) or chronic idiopathic urticaria. Please print and complete the forms below. Moderate to severe persistent asthma in people 6. Web patient enrollment and consent form xolair® (omalizumab) is indicated for: View and track your patient cases; Genentech patient foundation provides free medicine to patients without. Web xhale+ program patient enrolment and consent form:
• adult and pediatric patients (6 years of age and above) with moderate to severe persistent asthma. View benefits investigation (bi) reports; In order to make appropriate medical necessity determinations,. Patient’s first name last name middle initial date of birth prescriber’s first. (1) documentation of positive clinical response to xolair therapy authorization will be issued for 12 months. Moderate to severe persistent asthma in people 6. Web this service offers coverage support, patient assistance, and other useful information. Web with my patient solutions, you can: See full prescribing, safety, & boxed warning info. Web 1 of 2 prescription & enrollment form:
Web xolair® (omalizumab) enrollment form xolair® (omalizumab) enrollment form fax completed form to: Web find xolair® (omalizumab) support for our practice, including financial supports, billing and distribution information, office support materials, & patient education resources. Web with my patient solutions, you can: Committed to helping patients access the xolair they have been prescribed. Blue cross and blue shield of texas. The bias introduced by allowing enrollment of patients previously exposed to. For patients prescribed prxolair® for moderate to severe allergic asthma (aa) or chronic idiopathic urticaria. Please print and complete the forms below. In order to make appropriate medical necessity determinations,. Web sign up to receive patient support resources, including information on getting started with xolair® (omalizumab).
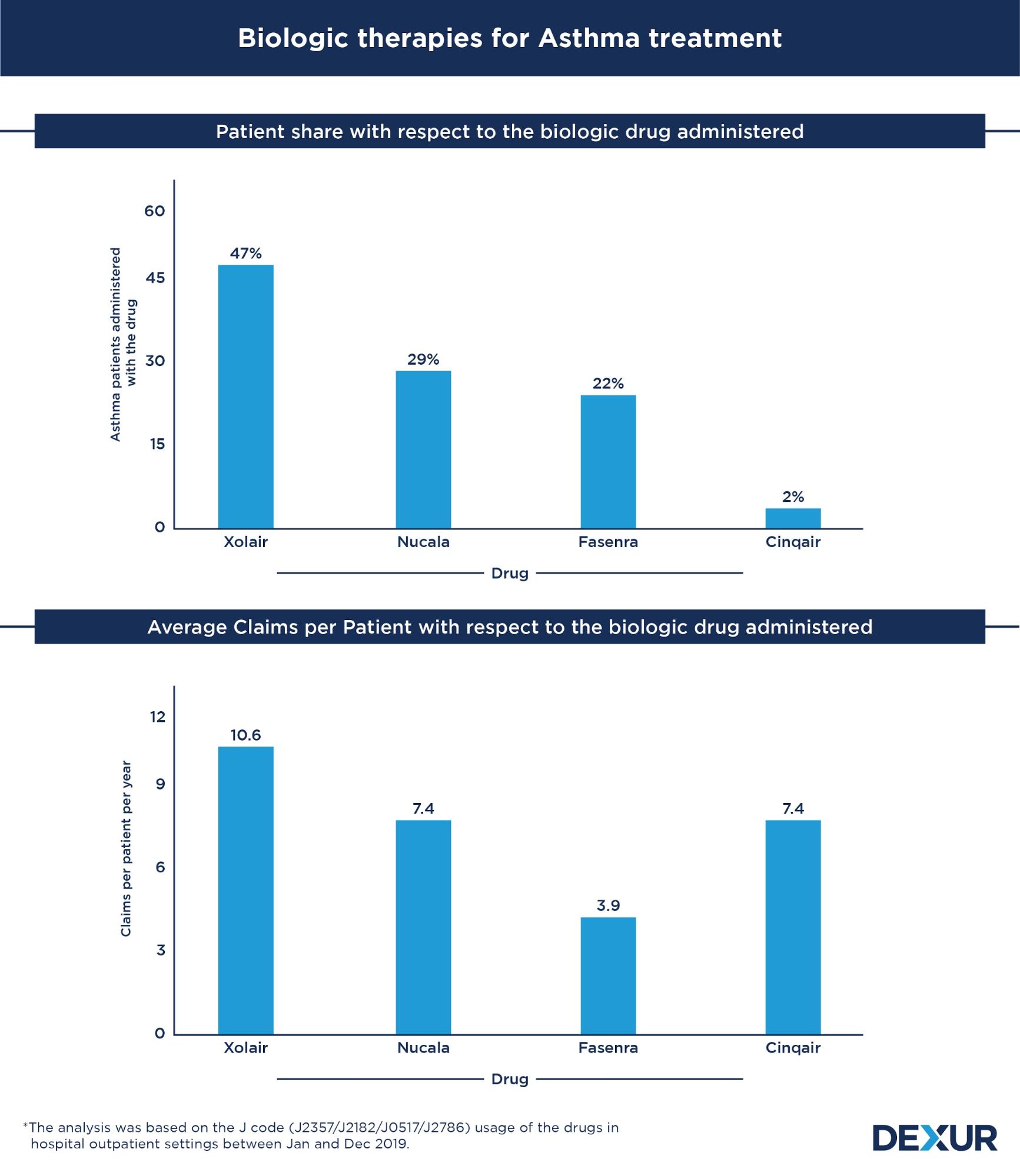
Xolair patient share was 1.6x more than Nucala and 2x compared to
See full prescribing, safety, & boxed warning info. Web the xolair recertification reminder program helps eligible patients avoid potential gaps in their xolair therapy due to insurance recertification requirements. View and track your patient cases; Xolair ® (omalizumab) for subcutaneous use is an injectable prescription medicine used to treat: Web xolair will be approved based on the following criterion:
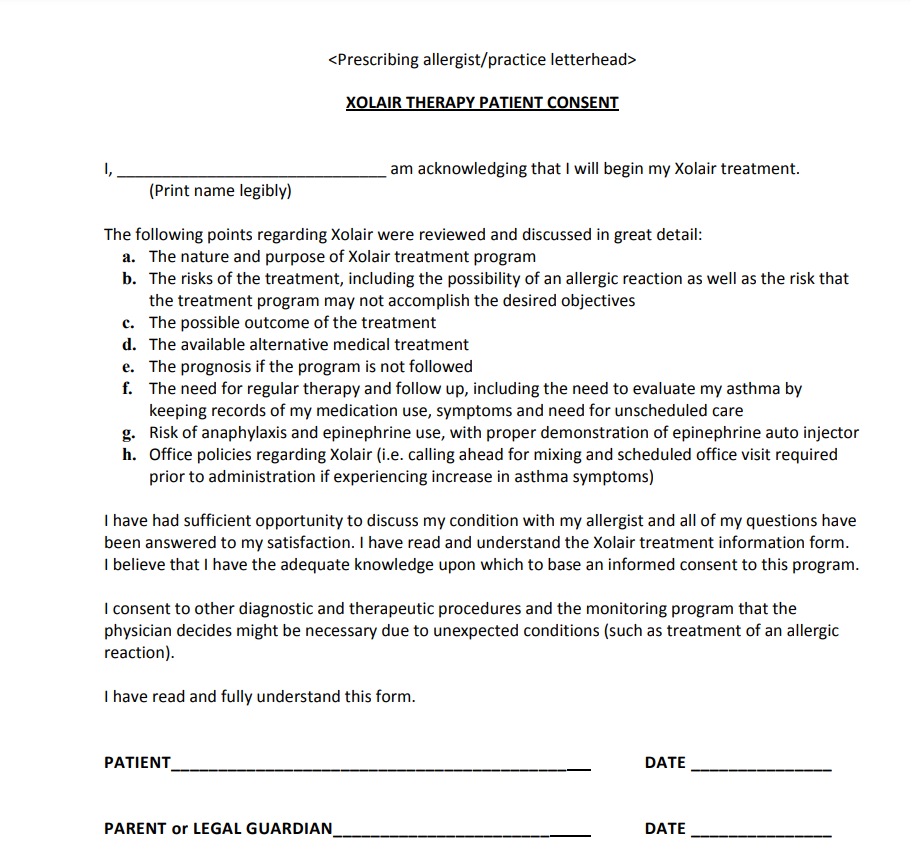
Xolair Patient Consent Form 2023
In order to make appropriate medical necessity determinations,. Your patient’s benefit plan requires prior authorization for certain medications. Blue cross and blue shield of texas. Committed to helping patients access the xolair they have been prescribed. Web find xolair® (omalizumab) support for our practice, including financial supports, billing and distribution information, office support materials, & patient education resources.
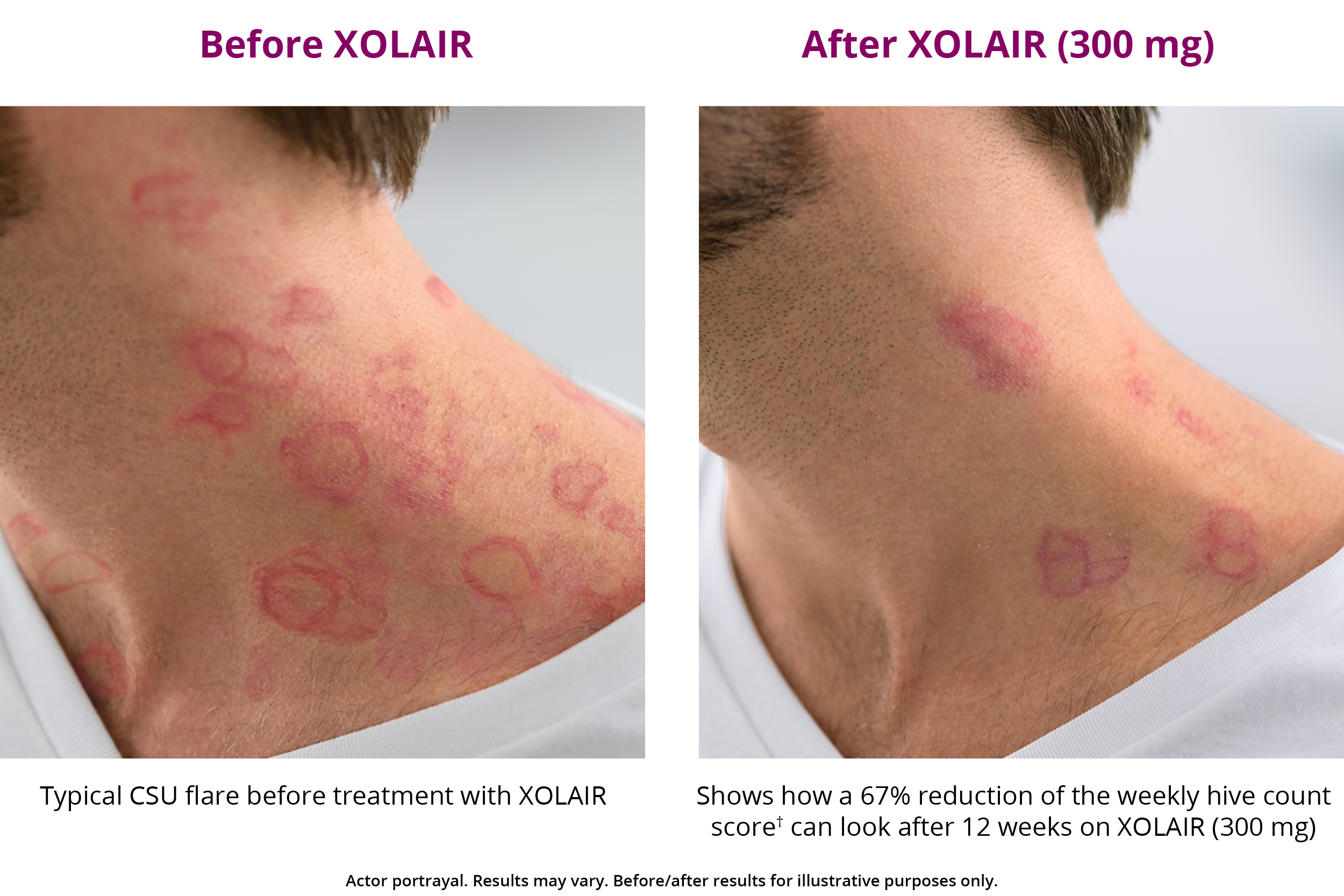
XOLAIR CSU Treatment Results XOLAIR® (omalizumab)
Genentech patient foundation provides free medicine to patients without. Web patient enrollment and consent form for patients prescribed prxolair® for chronic idiopathic urticaria (ciu), all sections must be completely filled out (please print). Your patient’s benefit plan requires prior authorization for certain medications. (1) documentation of positive clinical response to xolair therapy authorization will be issued for 12 months. View.

XOLAIR Dosage & Rx Info Uses, Side Effects MPR
Patient’s first name last name middle initial date of birth prescriber’s first. See full prescribing, safety, & boxed warning info. Web xhale+ program patient enrolment and consent form: Web download the forbearing consent form to begin enrollment with xolair access solutions. Committed to helping patients access the xolair they have been prescribed.
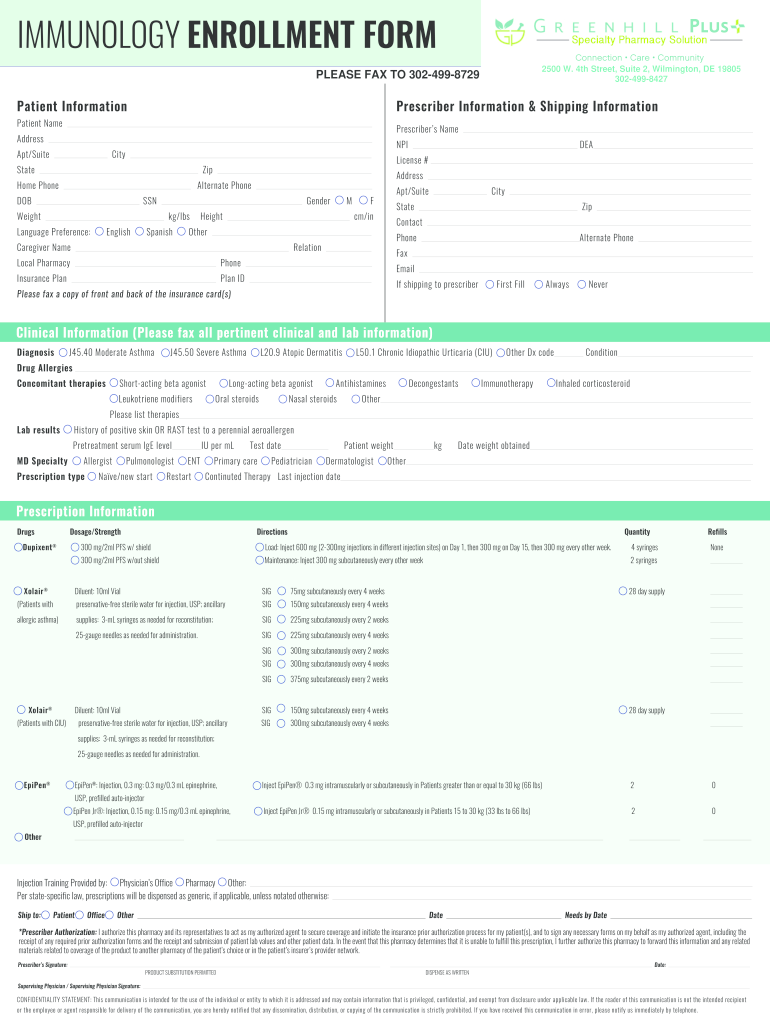
Xolair Enrollment Form Enrollment Form
Ad proudly helping members navigate prescription assistance programs for 15 years! Web xolair® (omalizumab) enrollment form xolair® (omalizumab) enrollment form fax completed form to: Moderate to severe persistent asthma in people 6. Blue cross and blue shield of texas. Web patient enrollment and consent form for patients prescribed prxolair® for chronic idiopathic urticaria (ciu), all sections must be completely filled.

Xhale+ Xolair Enrolment Consent Form Cloud Practice
Web download of patient consent form to begin enrollment with xolair admittance choose. In order to make appropriate medical necessity determinations,. Please print and complete the forms below. See full prescribing, safety, & boxed warning info. Web patient enrollment and consent form for patients prescribed prxolair® for chronic idiopathic urticaria (ciu), all sections must be completely filled out (please print).
Enrollment Form For Xolair Enrollment Form
See full prescribing, safety, & boxed warning info. Review the dosing schedule and your administration options. Committed to helping patients access the xolair they have been prescribed. View benefits investigation (bi) reports; Web patient enrollment forms | xolair access solutions forms and documents download the form you need to enroll in genentech access solutions.

Why Every Xolair Patient Should Keep an Allergy Journal IVX Health
Patient’s first name last name middle initial date of birth prescriber’s first. Once completed, fax to the number indicated on the form. Ad visit the patient site to learn how the fasenra pen works. Your patient’s benefit plan requires prior authorization for certain medications. In order to make appropriate medical necessity determinations,.

Xolair Dose Table Wallseat.co
Once completed, fax to the number indicated on the form. Please print and complete the forms below. View benefits investigation (bi) reports; The bias introduced by allowing enrollment of patients previously exposed to. See full prescribing, safety, & boxed warning info.
Chronic Spontaneous Urticaria Treatment XOLAIR® (omalizumab)
Web xolair® (omalizumab) enrollment form xolair® (omalizumab) enrollment form fax completed form to: In order to make appropriate medical necessity determinations,. Once completed, fax to the number indicated on the form. Web the xolair recertification reminder program helps eligible patients avoid potential gaps in their xolair therapy due to insurance recertification requirements. Web this service offers coverage support, patient assistance,.
Ad Proudly Helping Members Navigate Prescription Assistance Programs For 15 Years!
Moderate to severe persistent asthma in people 6. Web xolair will be approved based on the following criterion: Patient’s first name last name middle initial date of birth prescriber’s first. Committed to helping patients access the xolair they have been prescribed.
Web Xhale+ Program Patient Enrolment And Consent Form:
(1) documentation of positive clinical response to xolair therapy authorization will be issued for 12 months. Web find xolair® (omalizumab) support for our practice, including financial supports, billing and distribution information, office support materials, & patient education resources. Web the first step is to have patients complete and submit the respiratory patient consent form. Xolair® (omalizumab) fax completed form to 866.531.1025.
Web Patient Enrollment And Consent Form Xolair® (Omalizumab) Is Indicated For:
• adult and pediatric patients (6 years of age and above) with moderate to severe persistent asthma. Web patient enrollment and consent form for patients prescribed prxolair® for chronic idiopathic urticaria (ciu), all sections must be completely filled out (please print). Genentech patient foundation provides free medicine to patients without. Ad visit the patient site to learn how the fasenra pen works.
Web The Xolair Recertification Reminder Program Helps Eligible Patients Avoid Potential Gaps In Their Xolair Therapy Due To Insurance Recertification Requirements.
Web 1 of 2 prescription & enrollment form: For patients prescribed prxolair® for moderate to severe allergic asthma (aa) or chronic idiopathic urticaria. Please print and complete the forms below. Web this service offers coverage support, patient assistance, and other useful information.