Workers Compensation C2 Form
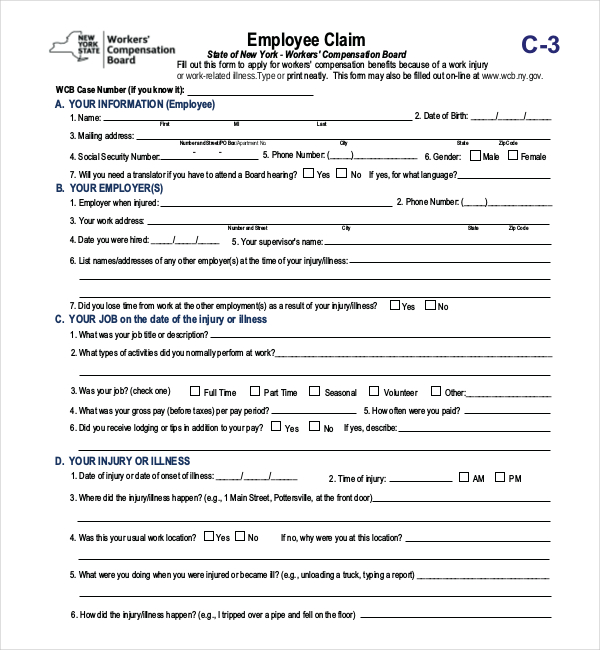
Workers Compensation C2 Form - Web ecomp submit forms online through the employees' compensation operations and management portal (ecomp). This form can be completed and printed via the link below, or also. Web date/hours of employment and wages. Web it is the responsibility of the employer to submit the c2 form by documenting it in the payroll portal for you to receive an indexed carrier case number from the city of new york law. The form, titled “employer’s first report of. Web workers' compensation program forms. Web nys workers' compensation insurance coverage. (print name of authorized representative or licensed agent of insurance carrier) title:. Web the c2, or an alternative report of injury document, must be completed within 10 days of the injury/illness or be subject to a penalty by the new york workers’. Web world trade center volunteer's claim for compensation.
Web ecomp submit forms online through the employees' compensation operations and management portal (ecomp). Web workers' compensation forms and worksheets. This form can be completed and printed via the link below, or also. Occupational disease claim form continuation of pay excused absence medical treatment return to work (employee). Date, time and location of injury. Web workers' compensation program forms. Web date/hours of employment and wages. Home address and phone number. (print name of authorized representative or licensed agent of insurance carrier) title:. The form, titled “employer’s first report of.
(print name of authorized representative or licensed agent of insurance carrier) title:. Web the c2, or an alternative report of injury document, must be completed within 10 days of the injury/illness or be subject to a penalty by the new york workers’. The form, titled “employer’s first report of. Home address and phone number. Web workers' compensation program forms. Web date/hours of employment and wages. Web world trade center volunteer's claim for compensation. Web it is the responsibility of the employer to submit the c2 form by documenting it in the payroll portal for you to receive an indexed carrier case number from the city of new york law. Web refer to this step by step process to file your claim. Web ecomp submit forms online through the employees' compensation operations and management portal (ecomp).

C2 Form Fill Online, Printable, Fillable, Blank pdfFiller
Web date/hours of employment and wages. Volunteer worker who suffered injury/illness at or near the world trade center (ground zero) or the fresh kills landfill. (print name of authorized representative or licensed agent of insurance carrier) title:. Web nys workers' compensation insurance coverage. This form can be completed and printed via the link below, or also.

For the workers’ compensation system, the election were good.
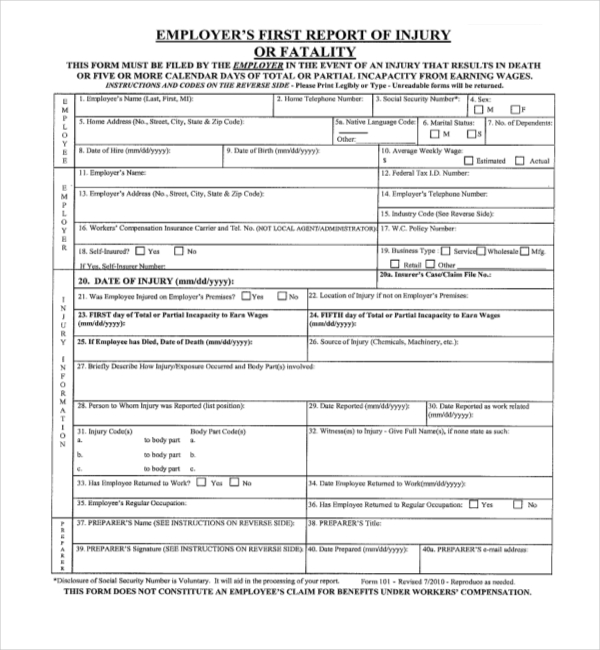
Date, time and location of injury. Web workers' compensation program forms. (print name of authorized representative or licensed agent of insurance carrier) title:. The form, titled “employer’s first report of. Web it is the responsibility of the employer to submit the c2 form by documenting it in the payroll portal for you to receive an indexed carrier case number from.

Workers' Compensation Claim Form California Free Download
(print name of authorized representative or licensed agent of insurance carrier) title:. The form, titled “employer’s first report of. Web the c2, or an alternative report of injury document, must be completed within 10 days of the injury/illness or be subject to a penalty by the new york workers’. Web world trade center volunteer's claim for compensation. Date, time and.
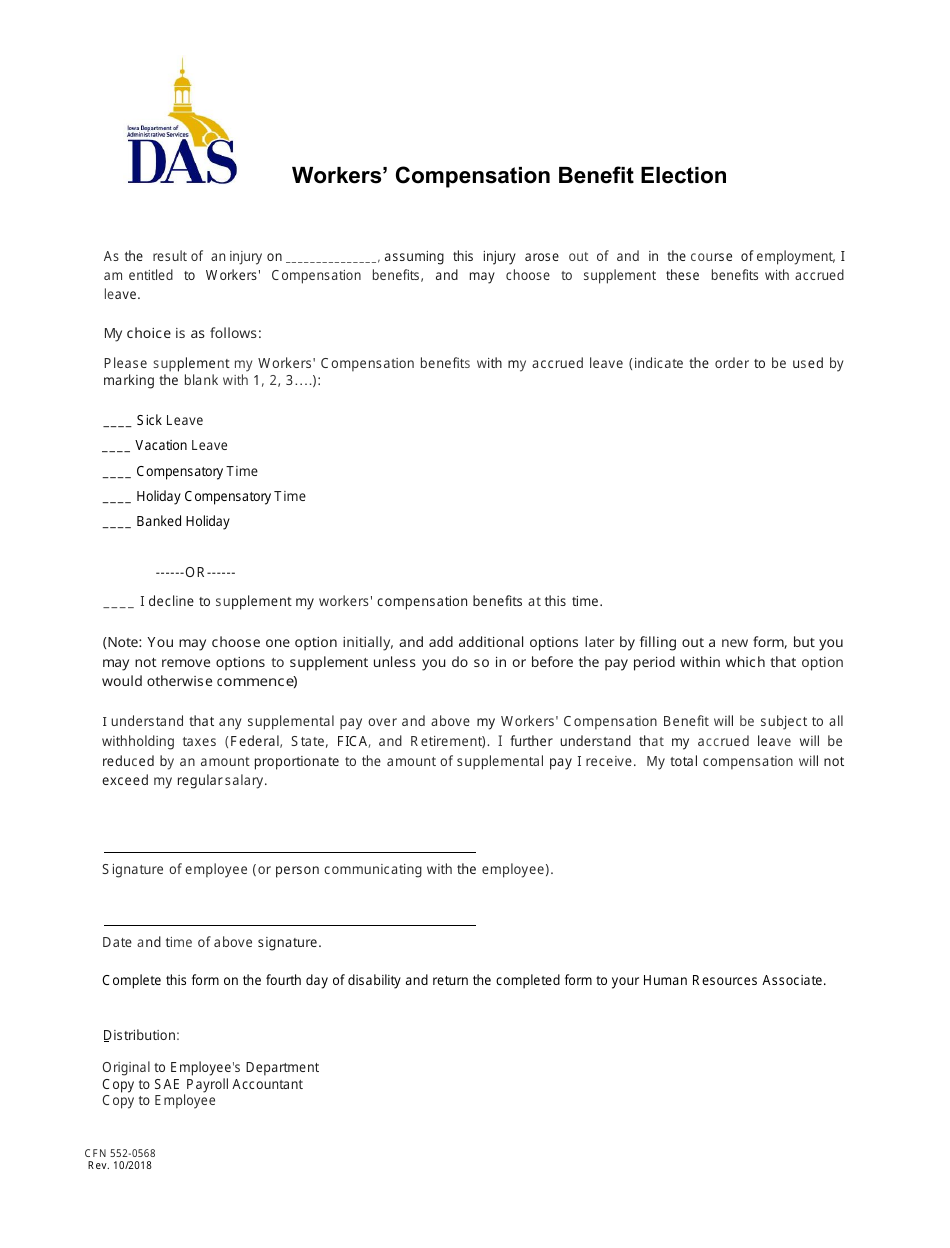
Form CFN5520568 Download Printable PDF or Fill Online Workers
Web workers' compensation forms and worksheets. Web refer to this step by step process to file your claim. (print name of authorized representative or licensed agent of insurance carrier) title:. Web the c2, or an alternative report of injury document, must be completed within 10 days of the injury/illness or be subject to a penalty by the new york workers’..
37+ truck accident settlement calculator GraceKalvin
On the ecomp site you can register for an account,. Date, time and location of injury. Web nys workers' compensation insurance coverage. Web the c2, or an alternative report of injury document, must be completed within 10 days of the injury/illness or be subject to a penalty by the new york workers’. (print name of authorized representative or licensed agent.

Wrongful Termination after Workers’ Compensation Claim Lewisville, TX
Volunteer worker who suffered injury/illness at or near the world trade center (ground zero) or the fresh kills landfill. On the ecomp site you can register for an account,. Web ecomp submit forms online through the employees' compensation operations and management portal (ecomp). Web it is the responsibility of the employer to submit the c2 form by documenting it in.
Workers Compensation Form Ce 200 Form Resume Examples 0g27XBq9Pr
Occupational disease claim form continuation of pay excused absence medical treatment return to work (employee). Web the c2, or an alternative report of injury document, must be completed within 10 days of the injury/illness or be subject to a penalty by the new york workers’. Home address and phone number. Web world trade center volunteer's claim for compensation. The form,.
FREE 13+ Sample Workers Compensation Forms in PDF XLS Word
(print name of authorized representative or licensed agent of insurance carrier) title:. Web date/hours of employment and wages. Web workers' compensation program forms. Home address and phone number. Web workers' compensation forms and worksheets.

Workers' Compensation Claim Form California Free Download
Home address and phone number. Web the c2, or an alternative report of injury document, must be completed within 10 days of the injury/illness or be subject to a penalty by the new york workers’. Web it is the responsibility of the employer to submit the c2 form by documenting it in the payroll portal for you to receive an.

Workers' Compensation Form Massachusetts Free Download
Web ecomp submit forms online through the employees' compensation operations and management portal (ecomp). Web workers' compensation forms and worksheets. On the ecomp site you can register for an account,. Web date/hours of employment and wages. The form, titled “employer’s first report of.
Home Address And Phone Number.
Web workers' compensation program forms. The form, titled “employer’s first report of. Web date/hours of employment and wages. On the ecomp site you can register for an account,.
Web Nys Workers' Compensation Insurance Coverage.
Web workers' compensation forms and worksheets. Web refer to this step by step process to file your claim. Date, time and location of injury. Web it is the responsibility of the employer to submit the c2 form by documenting it in the payroll portal for you to receive an indexed carrier case number from the city of new york law.
Web Ecomp Submit Forms Online Through The Employees' Compensation Operations And Management Portal (Ecomp).
This form can be completed and printed via the link below, or also. Web world trade center volunteer's claim for compensation. Volunteer worker who suffered injury/illness at or near the world trade center (ground zero) or the fresh kills landfill. Web the c2, or an alternative report of injury document, must be completed within 10 days of the injury/illness or be subject to a penalty by the new york workers’.
(Print Name Of Authorized Representative Or Licensed Agent Of Insurance Carrier) Title:.
Occupational disease claim form continuation of pay excused absence medical treatment return to work (employee).