Vns Referral Form Pdf
Vns Referral Form Pdf - Refer a patient to hospice care refer a patient online refer a patient by phone refer a patient by fax submit hospice referrals online. I am a medicare pecos enrolled physician and i certify that: Web by referring your patient to vns health, you can know that they will be treated with dignity and compassion — every single day. Web vns health referral form phone referral and inquiries: You can find credentialing forms by clicking on this link. Here you can find forms to join our network, update your demographic information, get prior authorizations for a patient’s medications, and more. Vnshealth.org/hospicereferral referral source date/time of referral referrer tel # source: To make a referral to vnsny choice mltc: 914.682.1480 fax referral form to: Web for all patients clinical status supports the need for the following skilled services/tasks:
914.682.1480 fax referral form to: _____ for home health service under medicare: Web vns health referral form phone referral and inquiries: Vnshealth.org/hospicereferral referral source date/time of referral referrer tel # source: Web for all patients clinical status supports the need for the following skilled services/tasks: 914.682.1488 patient information name telephone ( ) 5. You can find credentialing forms by clicking on this link. If you prefer, you can download our referral form and email it to [email protected] or fax it to 1. Hospital/snf (name/unit #) md pt/fam other adult care team # mrn # patient information patient name gender m f language spoken address tel # Web hospice referral form tel:
If you prefer, you can download our referral form and email it to [email protected] or fax it to 1. Services requested sn r pt r hha r ot r st r msw Hospital/snf (name/unit #) md pt/fam other adult care team # mrn # patient information patient name gender m f language spoken address tel # _____ for home health service under medicare: Expedited ‐ member faces imminent and serious threat to life or health; Web for all patients clinical status supports the need for the following skilled services/tasks: Skilled nursing care physical therapy occupational therapy speech/language therapy certifying physician signature print physician name phone address fax date / / 914.682.1488 patient information name telephone ( ) 5. Request for home care services referral form: Web hospice referral form tel:
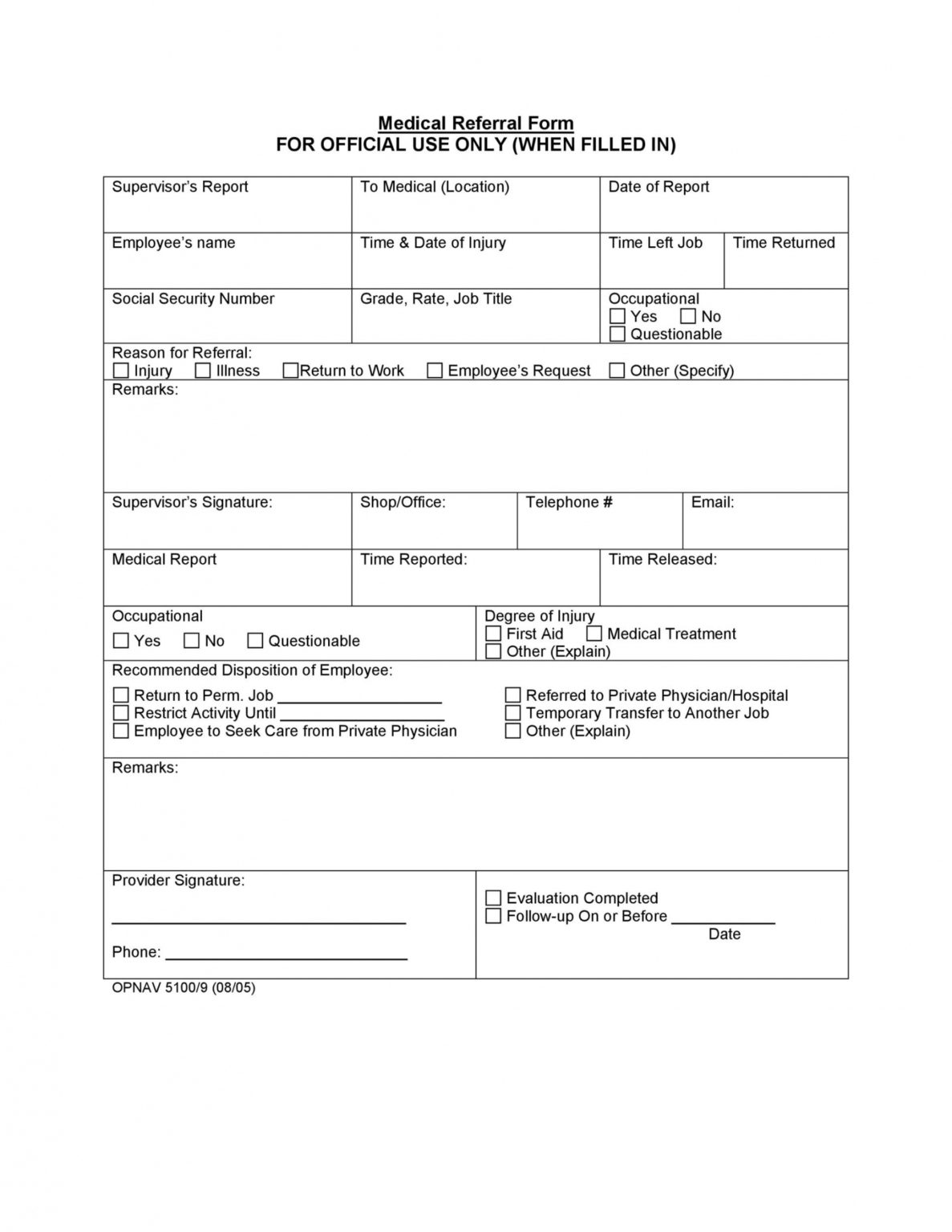
Medical Referral Form templates free printable
Expedited ‐ member faces imminent and serious threat to life or health; 914.682.1488 patient information name telephone ( ) 5. Here you can find forms to join our network, update your demographic information, get prior authorizations for a patient’s medications, and more. If you prefer, you can download our referral form and email it to [email protected] or fax it to.

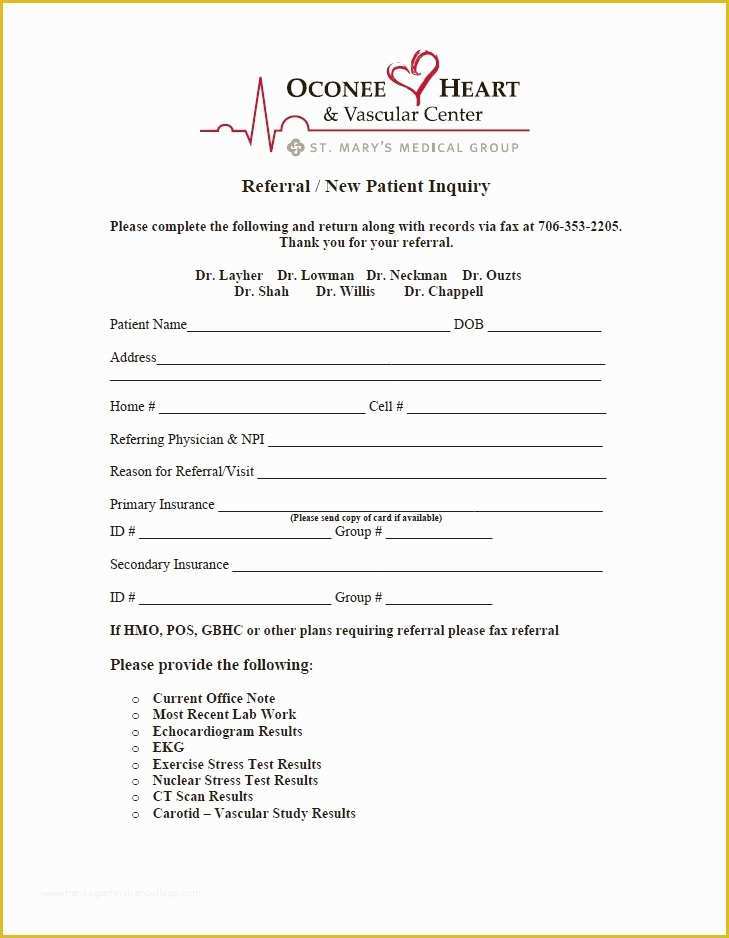
Information for Referring Doctors Indiana Nephrology
If you prefer, you can download our referral form and email it to [email protected] or fax it to 1. Request for home care services referral form: Here you can find forms to join our network, update your demographic information, get prior authorizations for a patient’s medications, and more. Skilled nursing care physical therapy occupational therapy speech/language therapy certifying physician signature.

(1) Knowledge Base
Web hospice referral form tel: _____ for home health service under medicare: Web by referring your patient to vns health, you can know that they will be treated with dignity and compassion — every single day. Hospital/snf (name/unit #) md pt/fam other adult care team # mrn # patient information patient name gender m f language spoken address tel #.
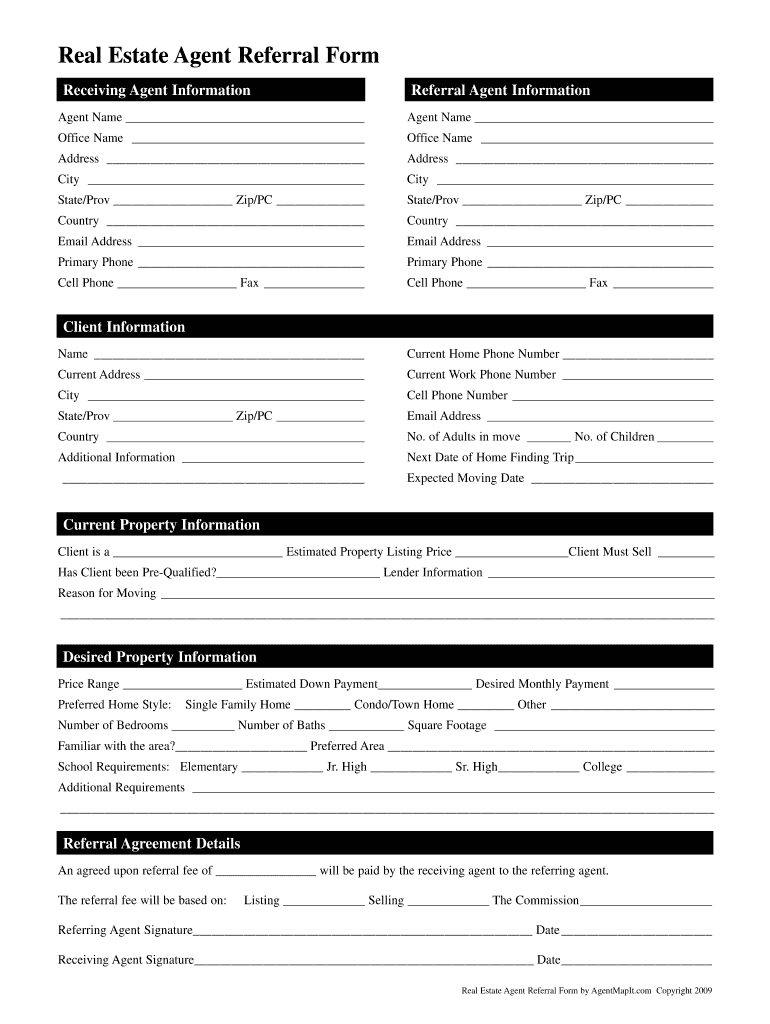
Referral Form Sample Download The Document Template
Please note the following definitions and timeframes for processing requests: Here you can find forms to join our network, update your demographic information, get prior authorizations for a patient’s medications, and more. 914.682.1488 patient information name telephone ( ) 5. Web by referring your patient to vns health, you can know that they will be treated with dignity and compassion.

ExitPolls
914.682.1480 fax referral form to: Skilled nursing care physical therapy occupational therapy speech/language therapy certifying physician signature print physician name phone address fax date / / Request for home care services referral form: Refer a patient to hospice care refer a patient online refer a patient by phone refer a patient by fax submit hospice referrals online. Web forms for.
Sample 50 Referral Form Templates Medical & General ᐅ Templatelab
Request for home care services referral form: Hospital/snf (name/unit #) md pt/fam other adult care team # mrn # patient information patient name gender m f language spoken address tel # Web by referring your patient to vns health, you can know that they will be treated with dignity and compassion — every single day. Web for all patients clinical.
Medical Referral form Template Free Of Medical Referral form
Vnshealth.org/hospicereferral referral source date/time of referral referrer tel # source: To make a referral to vnsny choice mltc: Skilled nursing care physical therapy occupational therapy speech/language therapy certifying physician signature print physician name phone address fax date / / Web by referring your patient to vns health, you can know that they will be treated with dignity and compassion —.
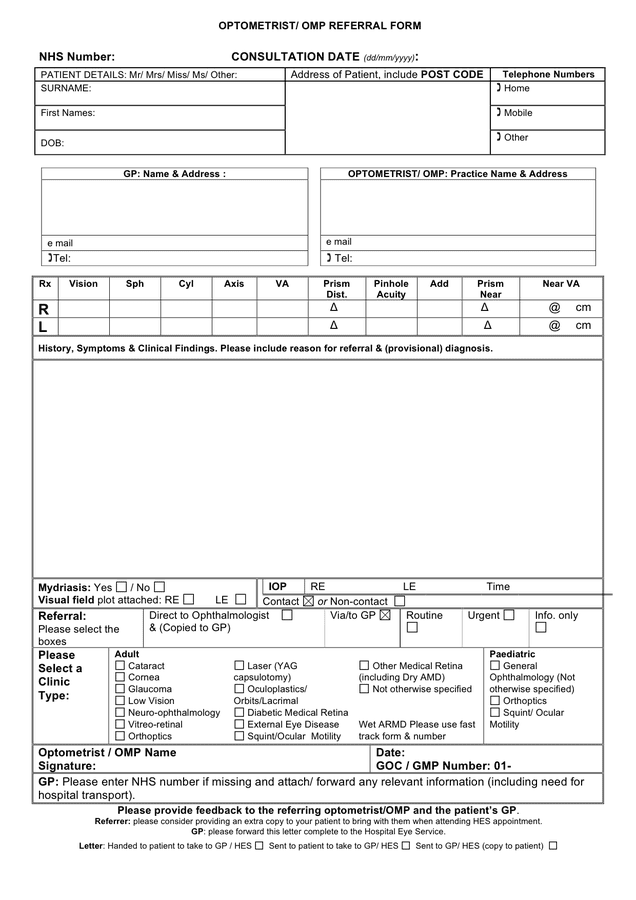
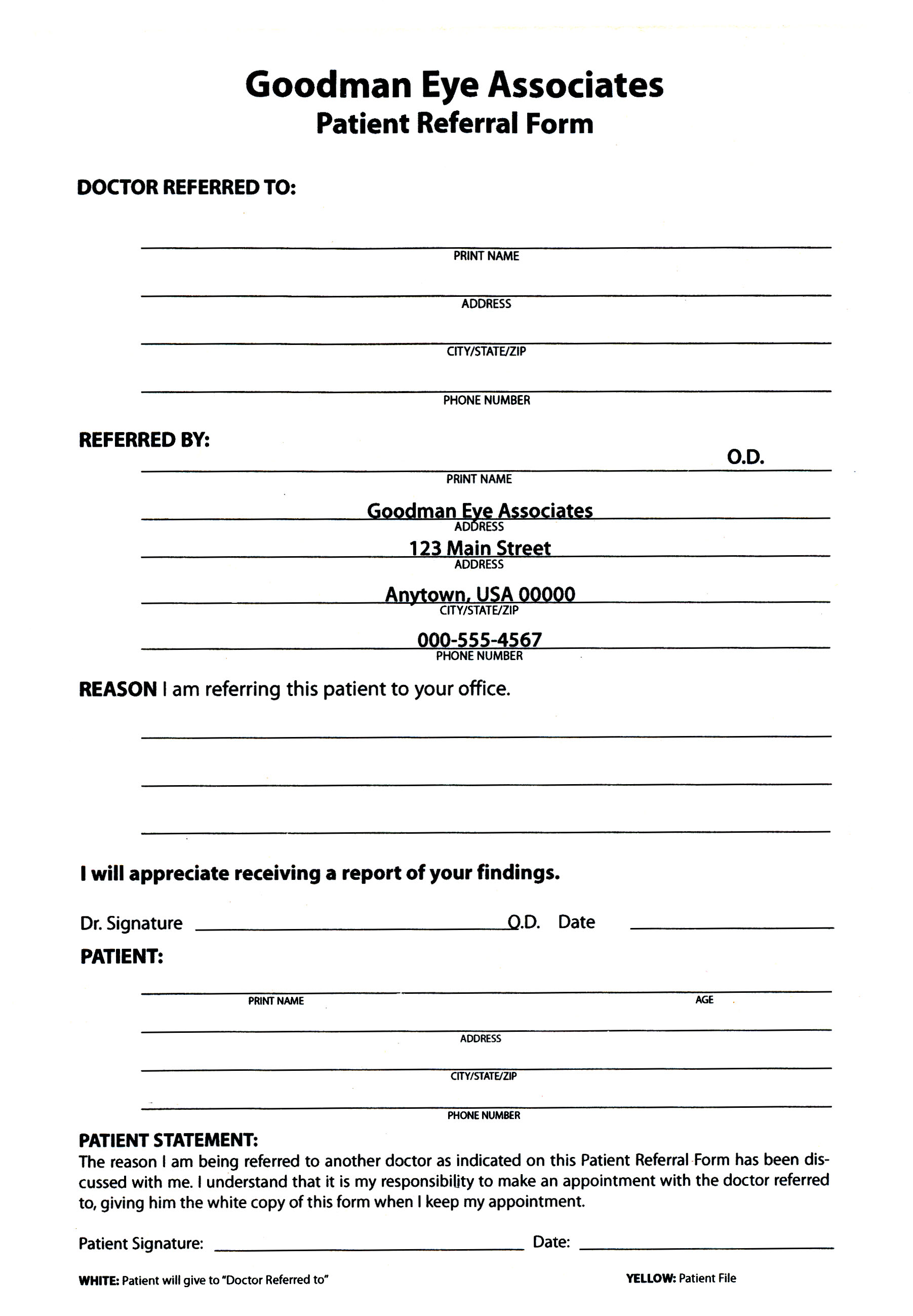
Optometrist referral form in Word and Pdf formats
Services requested sn r pt r hha r ot r st r msw Web for all patients clinical status supports the need for the following skilled services/tasks: Web vns health referral form phone referral and inquiries: Request for home care services referral form: Web by referring your patient to vns health, you can know that they will be treated with.
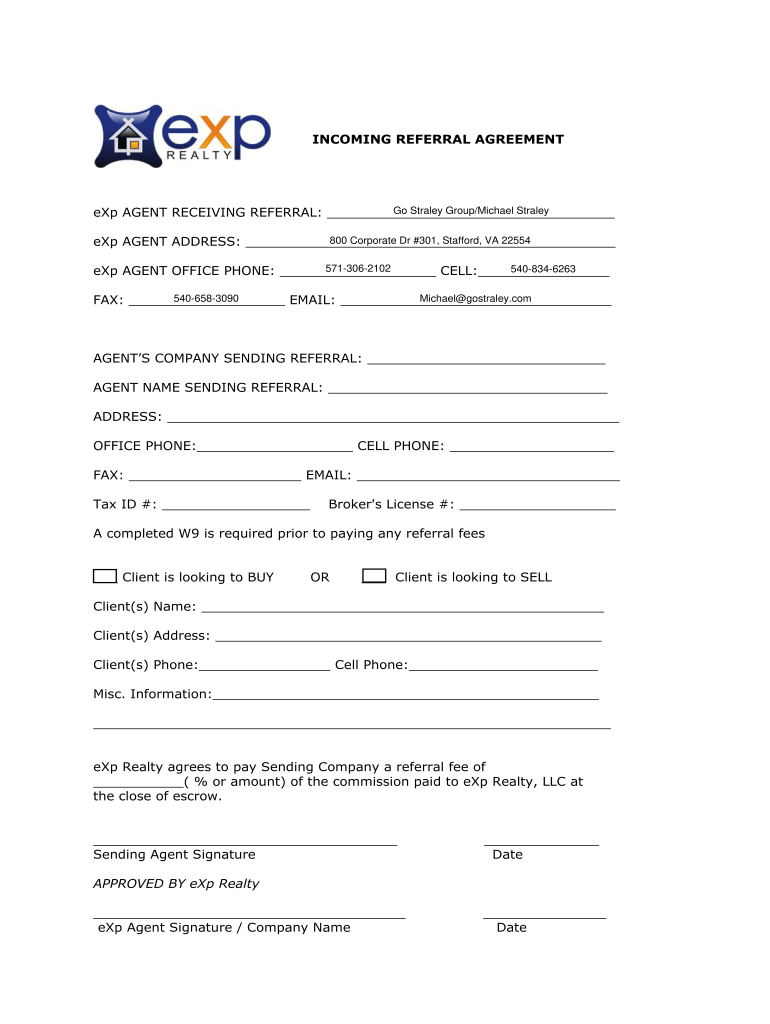
Exp Referral Form Fill Online, Printable, Fillable, Blank pdfFiller
If you prefer, you can download our referral form and email it to [email protected] or fax it to 1. To make a referral to vnsny choice mltc: Refer a patient to hospice care refer a patient online refer a patient by phone refer a patient by fax submit hospice referrals online. Web for all patients clinical status supports the need.
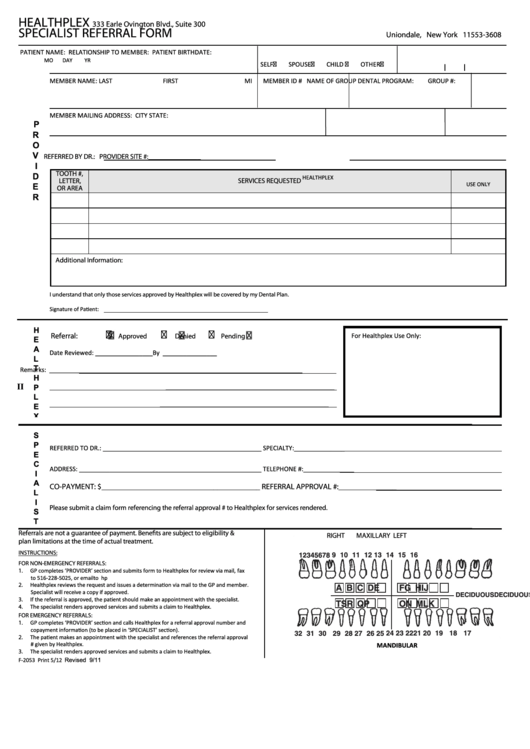
Dental Services Referral Form printable pdf download
Services requested sn r pt r hha r ot r st r msw You can find credentialing forms by clicking on this link. 914.682.1488 patient information name telephone ( ) 5. _____ for home health service under medicare: Vnshealth.org/hospicereferral referral source date/time of referral referrer tel # source:
914.682.1488 Patient Information Name Telephone ( ) 5.
Web vns health referral form phone referral and inquiries: Web please complete this form to request pre‐authorization from vnsny choice and fax it to the contact numbers at the bottom. Hospital/snf (name/unit #) md pt/fam other adult care team # mrn # patient information patient name gender m f language spoken address tel # I am a medicare pecos enrolled physician and i certify that:
To Make A Referral To Vnsny Choice Mltc:
Web by referring your patient to vns health, you can know that they will be treated with dignity and compassion — every single day. You can find credentialing forms by clicking on this link. This patient is confined to the home and needs intermittent skilled nursing care, physical. Web for all patients clinical status supports the need for the following skilled services/tasks:
Please Note The Following Definitions And Timeframes For Processing Requests:
Vnshealth.org/hospicereferral referral source date/time of referral referrer tel # source: Web hospice referral form tel: Skilled nursing care physical therapy occupational therapy speech/language therapy certifying physician signature print physician name phone address fax date / / _____ for home health service under medicare:
If You Prefer, You Can Download Our Referral Form And Email It To [email protected] Or Fax It To 1.
Expedited ‐ member faces imminent and serious threat to life or health; Web form may only be used in compliance with sdoh and vnsny choice guidelines. Request for home care services start of care date requested: Web forms for providers and patients.