Printable Hipaa Release Form
Printable Hipaa Release Form - Indicate his/her relationship to you.) _____ (print name of second parent or guardian; It must also include your health privacy rights. Web (print name of the parent or guardian; Your health care provider and health plan must give you a notice that tells you how they may use and share your health information. Indicate his/her relationship to you.) i understand that: Check the applicable box to indicate to whom you authorize the release of your medical info. Web a hipaa release form must be obtained from a patient before their protected health information is disclosed for any purpose other than those detailed in 45 cfr §164.506, which are specifically covered in 45 cfr §164.508 and summarized below: The release also allows the added option for healthcare providers to share information. To fill out a hipaa release form, a patient must choose the appropriate document. Web what is the hipaa notice i receive from my doctor and health plan?
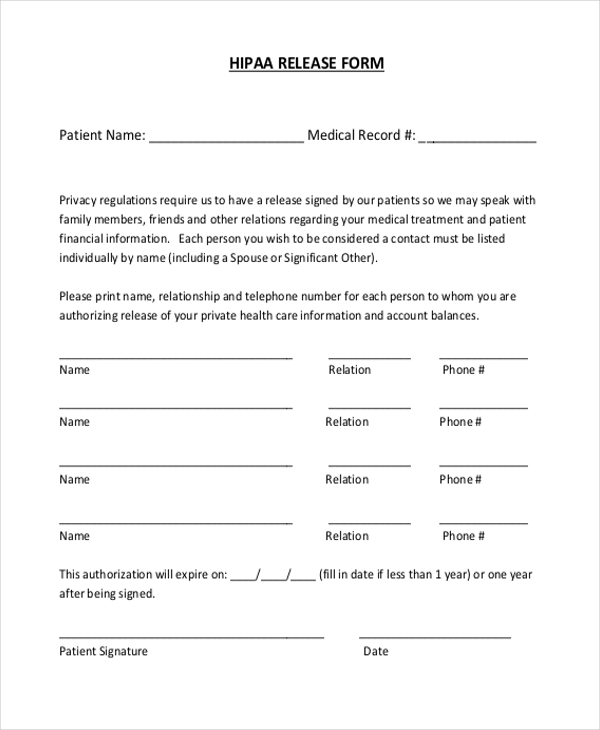
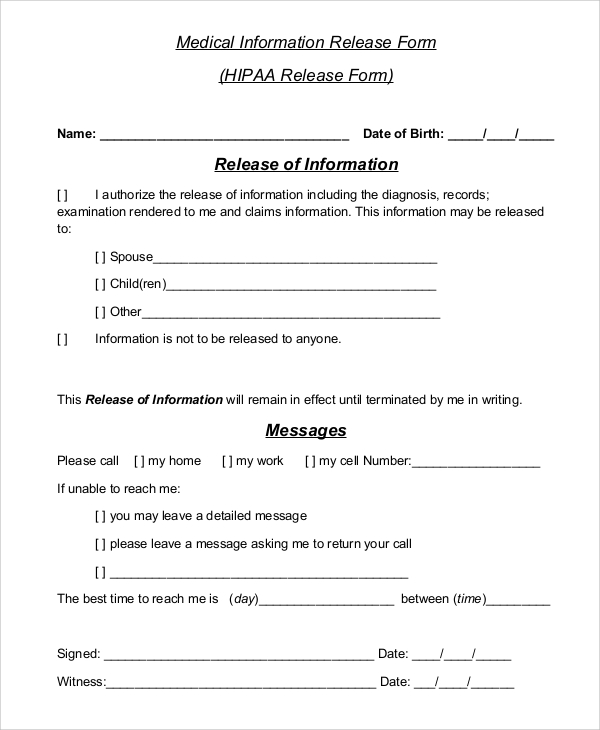
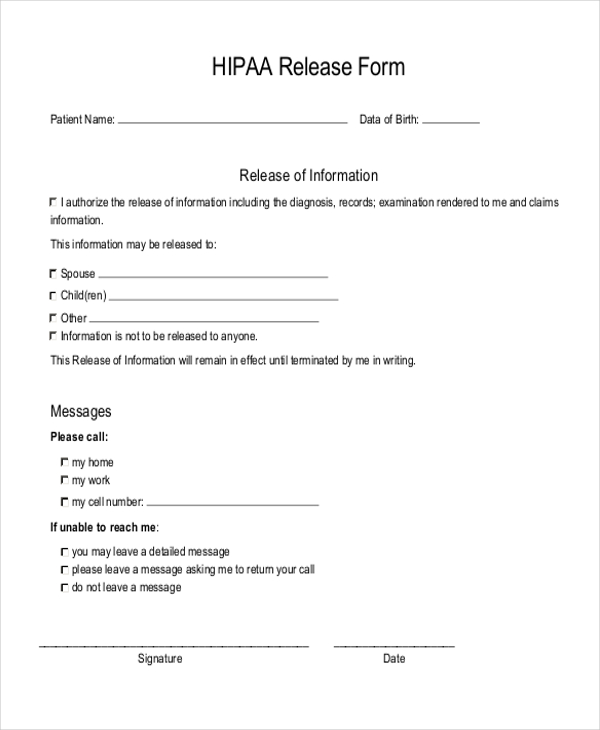
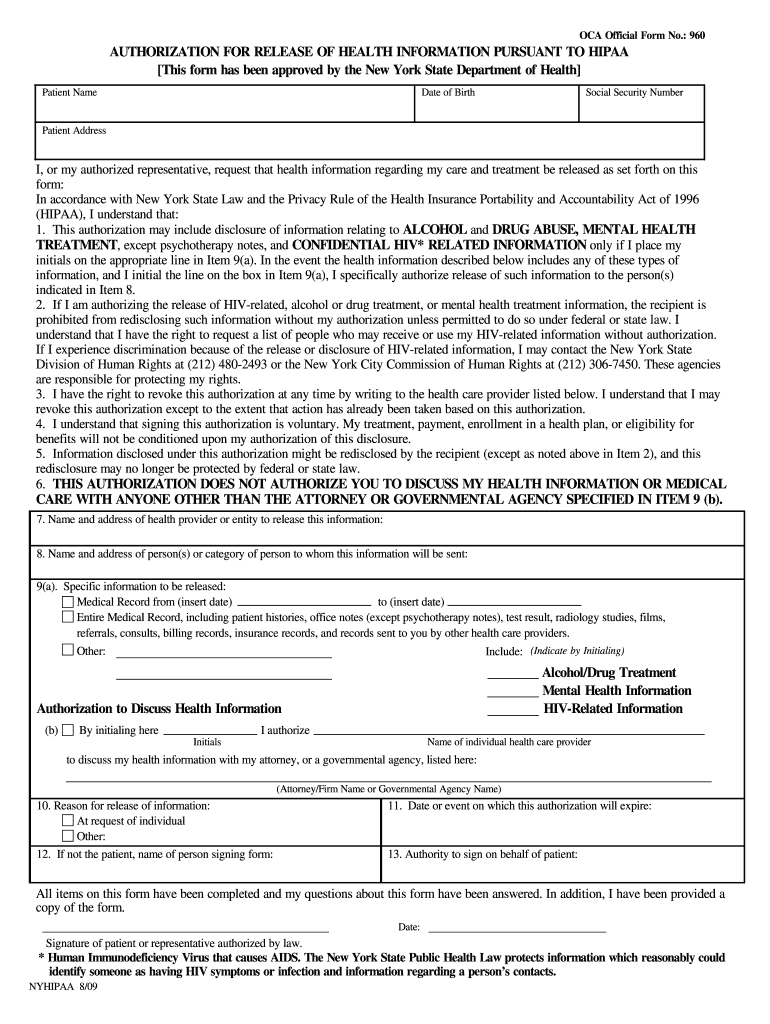
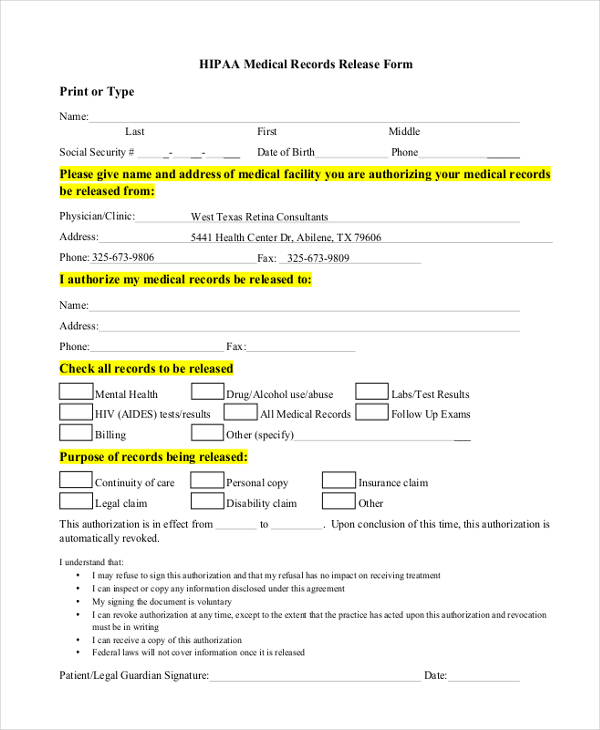
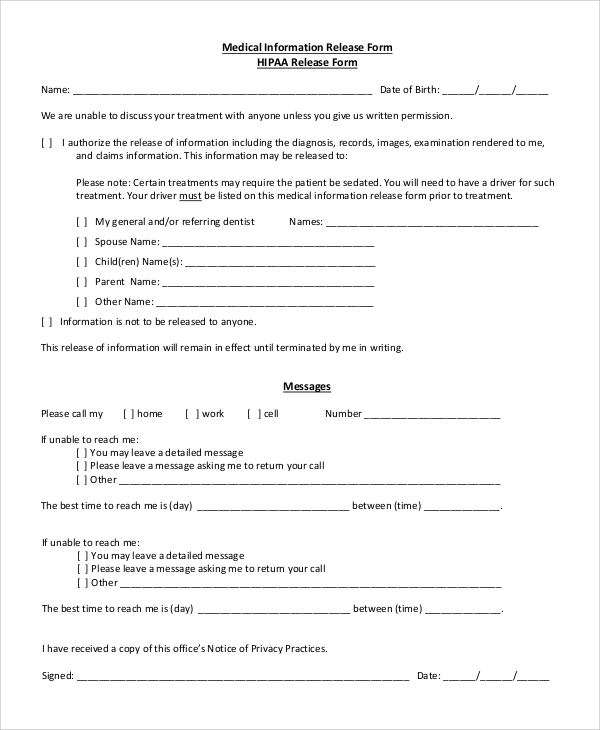
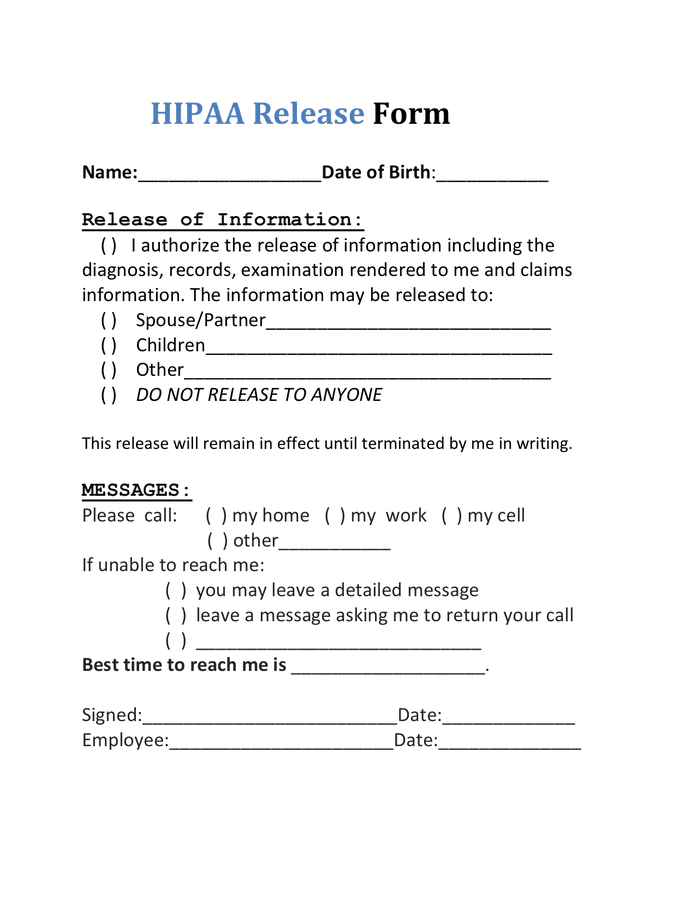
Indicate his/her relationship to you.) i understand that: Check the applicable box to indicate to whom you authorize the release of your medical info. To fill out a hipaa release form, a patient must choose the appropriate document. A medical release form can be revoked or reassigned at any time by the patient. Your health care provider and health plan must give you a notice that tells you how they may use and share your health information. Hipaa medical release authorization form. Web how to fill out a hipaa release form. Web a hipaa release form must be obtained from a patient before their protected health information is disclosed for any purpose other than those detailed in 45 cfr §164.506, which are specifically covered in 45 cfr §164.508 and summarized below: Web hipaa release form please complete all sections of this hipaa release form. In accordance with new york state law and the privacy rule of the health insurance portability and accountability act of 1996 (hipaa), i u.
Learn your rights under hipaa, how your information may be used or shared, and how to file a complaint if you think your rights were violated. Web hipaa for individuals. A medical release form can be revoked or reassigned at any time by the patient. Hipaa medical release authorization form. To fill out a hipaa release form, a patient must choose the appropriate document. The release also allows the added option for healthcare providers to share information. Web hipaa release form please complete all sections of this hipaa release form. Web patient name date of birth social security number patient address i, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form: Web a hipaa release form must be obtained from a patient before their protected health information is disclosed for any purpose other than those detailed in 45 cfr §164.506, which are specifically covered in 45 cfr §164.508 and summarized below: If any sections are left blank, this form will be invalid and it will not be possible for your health information to be shared as requested.
FREE 11+ Sample HIPAA Release Forms in PDF MS Word
Hipaa medical release authorization form. Your health care provider and health plan must give you a notice that tells you how they may use and share your health information. Web what is the hipaa notice i receive from my doctor and health plan? Web hipaa for individuals. The form must allow them to request their personal health information (phi) or.
Hipaa Compliant Medical Release Form amulette
If any sections are left blank, this form will be invalid and it will not be possible for your health information to be shared as requested. The release also allows the added option for healthcare providers to share information. Indicate his/her relationship to you.) i understand that: Hipaa medical release authorization form. Check the applicable box to indicate to whom.
FREE 8+ Sample Hipaa Release Forms in PDF MS Word
Web hipaa release form please complete all sections of this hipaa release form. To fill out a hipaa release form, a patient must choose the appropriate document. Indicate his/her relationship to you.) i understand that: Check the applicable box to indicate to whom you authorize the release of your medical info. Web patient name date of birth social security number.
FREE 11+ Sample HIPAA Release Forms in PDF MS Word
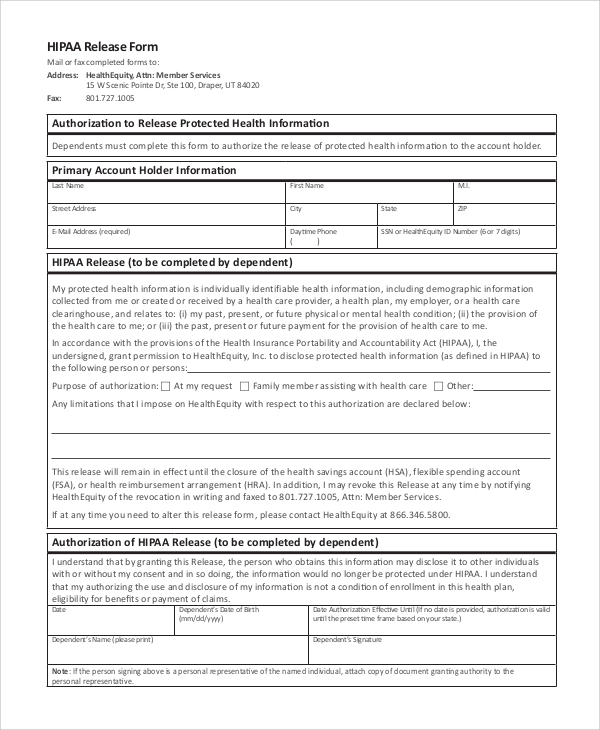
Your health care provider and health plan must give you a notice that tells you how they may use and share your health information. Hipaa medical release authorization form. Web the medical record information release (hipaa) form allows a patient to give authorization to a 3rd party and access their health records. Learn your rights under hipaa, how your information.
Hipaa Compliant Medical Release Form amulette
If any sections are left blank, this form will be invalid and it will not be possible for your health information to be shared as requested. Web how to fill out a hipaa release form. Web what is the hipaa notice i receive from my doctor and health plan? A medical release form can be revoked or reassigned at any.
Hipaa Release Form Example
The release also allows the added option for healthcare providers to share information. Web patient name date of birth social security number patient address i, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form: Web what is the hipaa notice i receive from my doctor and health plan?.
Hipaa Release Form Ny Fill Online, Printable, Fillable, Blank pdfFiller
The purpose is provided above so that i can make a decision as to whether to allow the release of information. Hipaa medical release authorization form. A medical release form can be revoked or reassigned at any time by the patient. Web what is the hipaa notice i receive from my doctor and health plan? Your health care provider and.
Hipaa Compliant Medical Release Form amulette
Web the medical record information release (hipaa) form allows a patient to give authorization to a 3rd party and access their health records. Web patient name date of birth social security number patient address i, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form: Adobe pdf, ms word,.
Hipaa Compliant Medical Release Form amulette
The purpose is provided above so that i can make a decision as to whether to allow the release of information. Adobe pdf, ms word, opendocument Your health care provider and health plan must give you a notice that tells you how they may use and share your health information. If any sections are left blank, this form will be.
HIPAA Release Form in Word and Pdf formats
Web a hipaa release form must be obtained from a patient before their protected health information is disclosed for any purpose other than those detailed in 45 cfr §164.506, which are specifically covered in 45 cfr §164.508 and summarized below: If any sections are left blank, this form will be invalid and it will not be possible for your health.
In Accordance With New York State Law And The Privacy Rule Of The Health Insurance Portability And Accountability Act Of 1996 (Hipaa), I U.
Web (print name of the parent or guardian; Web the medical record information release (hipaa) form allows a patient to give authorization to a 3rd party and access their health records. Web patient name date of birth social security number patient address i, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form: The form must allow them to request their personal health information (phi) or grant a third party permission to release it.
The Purpose Is Provided Above So That I Can Make A Decision As To Whether To Allow The Release Of Information.
If any sections are left blank, this form will be invalid and it will not be possible for your health information to be shared as requested. Hipaa medical release authorization form. Adobe pdf, ms word, opendocument Check the applicable box to indicate to whom you authorize the release of your medical info.
Web Hipaa For Individuals.
Your health care provider and health plan must give you a notice that tells you how they may use and share your health information. To fill out a hipaa release form, a patient must choose the appropriate document. Learn your rights under hipaa, how your information may be used or shared, and how to file a complaint if you think your rights were violated. Web hipaa release form please complete all sections of this hipaa release form.
It Must Also Include Your Health Privacy Rights.
Web what is the hipaa notice i receive from my doctor and health plan? Indicate his/her relationship to you.) _____ (print name of second parent or guardian; A medical release form can be revoked or reassigned at any time by the patient. Web a hipaa release form must be obtained from a patient before their protected health information is disclosed for any purpose other than those detailed in 45 cfr §164.506, which are specifically covered in 45 cfr §164.508 and summarized below: