Novo Nordisk Reorder Form
Novo Nordisk Reorder Form - Web novo nordisk refill formtures for signing a nova nor disk patient assistance application form in pdf format. Web service request form wegovy™ (semaglutide) injection 2.4 mgsaxenda® (liraglutide) injection 3 mg program phone: Novo nordisk does not accept paid. Web reorder form needs to be submitted: Use get form or simply click on the template preview to open it in the. After you have finished entering information, this form will be sent to your patient or their caregiver who. Web for households over 4, add $8,120 per person. New application, new documentation yearly : Needles will not be sent as part of the pap order if they are not requested. Web 800 scudders mill road plainsboro, nj 08536 tel:
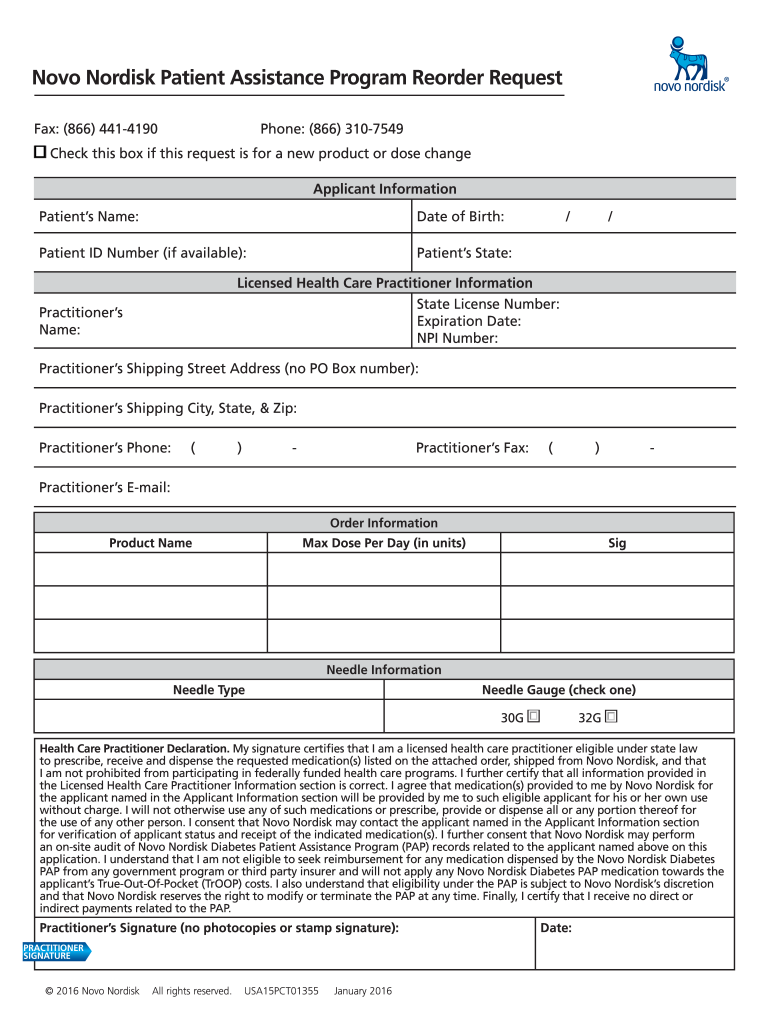
Web complete novo nordisk reorder form online with us legal forms. 24256790 transparency in employee health coverage: Use get form or simply click on the template preview to open it in the. Needles will not be sent as part of the pap order if they are not requested. New application, new documentation yearly : Signnow has paid close attention to ios users and developed an. Web i (or my parent/guardian/legal representative) agree that if i am (or the patient is) approved for pap as a medicare part d enrollee, that novo nordisk or pap may give my (or the. Web service request form wegovy™ (semaglutide) injection 2.4 mgsaxenda® (liraglutide) injection 3 mg program phone: Web reorder form needs to be submitted: Patient must not have insurance, or is enrolled in medicare.
Web novo nordisk refill formtures for signing a nova nor disk patient assistance application form in pdf format. Web for households over 4, add $8,120 per person. Needles will not be sent as part of the pap order if they are not requested. Web complete novo nordisk reorder form online with us legal forms. Web reorder form needs to be submitted: Novo nordisk does not accept paid. Web that novo nordisk may modify or terminate the pap at any time. Novo nordisk provides access to complimentary prescription medicine samples to eligible practitioners for appropriate patients. Use get form or simply click on the template preview to open it in the. Web service request form wegovy™ (semaglutide) injection 2.4 mgsaxenda® (liraglutide) injection 3 mg program phone:

Novo Nordisk to boost pillform diabetic drugs with 1.8 billion deal
Use get form or simply click on the template preview to open it in the. Novo nordisk does not accept paid. Web the information you enter will also be used for the novo nordisk compound sharing agreement (containing the information provided in the order form, the compound request. See “documents needed” on the next page for what constitutes acceptable proof.

Novo Nordisk and Friends for Diabetes form partnership to help curb
Patient must not have insurance, or is enrolled in medicare. 24256790 transparency in employee health coverage: Web for households over 4, add $8,120 per person. After you have finished entering information, this form will be sent to your patient or their caregiver who. Use get form or simply click on the template preview to open it in the.
Novo Nordisk Patient Assistance Refill Form 2020 Fill and Sign
Web i (or my parent/guardian/legal representative) agree that if i am (or the patient is) approved for pap as a medicare part d enrollee, that novo nordisk or pap may give my (or the. New application, new documentation yearly : Signnow has paid close attention to ios users and developed an. Novo nordisk provides access to complimentary prescription medicine samples.

Internship in Denmark OYA Opportunities
24256790 transparency in employee health coverage: Web 800 scudders mill road plainsboro, nj 08536 tel: Web those people who you authorize to speak to novo nordisk pap about you may provide or receive your personal information as necessary. Web please complete the sections below. Save or instantly send your ready documents.

Novo Nordisk Plans Valuebased Contracts For GLP1 Agonist Ozempic Scrip
Web that novo nordisk may modify or terminate the pap at any time. Needles will not be sent as part of the pap order if they are not requested. Patient must not have insurance, or is enrolled in medicare. Novo nordisk does not accept paid. New application, new documentation yearly :

novonordisk
Novo nordisk provides access to complimentary prescription medicine samples to eligible practitioners for appropriate patients. Needles will not be sent as part of the pap order if they are not requested. Web i (or my parent/guardian/legal representative) agree that if i am (or the patient is) approved for pap as a medicare part d enrollee, that novo nordisk or pap.

Contact Novo Nordisk our local offices
Web complete novo nordisk reorder form online with us legal forms. Patient must not have insurance, or is enrolled in medicare. Easily fill out pdf blank, edit, and sign them. Novo nordisk provides access to complimentary prescription medicine samples to eligible practitioners for appropriate patients. Web those people who you authorize to speak to novo nordisk pap about you may.
Dividende von Novo Nordisk im April 2021 Jung in Rente
Needles will not be sent as part of the pap order if they are not requested. Web reorder form needs to be submitted: Web i (or my parent/guardian/legal representative) agree that if i am (or the patient is) approved for pap as a medicare part d enrollee, that novo nordisk or pap may give my (or the. Save or instantly.

Headline results from Novo Nordisk's Pioneer trial
Web those people who you authorize to speak to novo nordisk pap about you may provide or receive your personal information as necessary. Web that novo nordisk may modify or terminate the pap at any time. Novo nordisk provides access to complimentary prescription medicine samples to eligible practitioners for appropriate patients. Web i (or my parent/guardian/legal representative) agree that if.

Novo Nordisk abre mais de 30 vagas Guia da Farmácia
Easily fill out pdf blank, edit, and sign them. Web for households over 4, add $8,120 per person. Needles will not be sent as part of the pap order if they are not requested. Use get form or simply click on the template preview to open it in the. Novo nordisk provides access to complimentary prescription medicine samples to eligible.
Web Complete Novo Nordisk Reorder Form Online With Us Legal Forms.
Novo nordisk provides access to complimentary prescription medicine samples to eligible practitioners for appropriate patients. See “documents needed” on the next page for what constitutes acceptable proof patients who are. Patient must not have insurance, or is enrolled in medicare. Web reorder form needs to be submitted:
Web The Information You Enter Will Also Be Used For The Novo Nordisk Compound Sharing Agreement (Containing The Information Provided In The Order Form, The Compound Request.
Save or instantly send your ready documents. Web 800 scudders mill road plainsboro, nj 08536 tel: Signnow has paid close attention to ios users and developed an. Needles will not be sent as part of the pap order if they are not requested.
Web Novo Nordisk Refill Formtures For Signing A Nova Nor Disk Patient Assistance Application Form In Pdf Format.
Web service request form wegovy™ (semaglutide) injection 2.4 mgsaxenda® (liraglutide) injection 3 mg program phone: New application, new documentation yearly : Web please complete the sections below. Web for households over 4, add $8,120 per person.
Easily Fill Out Pdf Blank, Edit, And Sign Them.
Web those people who you authorize to speak to novo nordisk pap about you may provide or receive your personal information as necessary. Use get form or simply click on the template preview to open it in the. Web i (or my parent/guardian/legal representative) agree that if i am (or the patient is) approved for pap as a medicare part d enrollee, that novo nordisk or pap may give my (or the. Patient must not have insurance, or is enrolled in medicare.