Medicare Claim Form 1490S
Medicare Claim Form 1490S - Web patient's request for medical payment. Send the form to the company that processes your medicare claims. They must also attach any bill ( s) they received from providers/suppliers. Web the claim and supporting documentation must be sent to the medicare administrative contractor (mac) responsible for the state in which you received the services. Web cms forms list. Get all forms in alternate formats. This is a commonly used form that will be submitted in order to request that a medical service be covered under medicare or medicaid. Forms get medicare forms for different situations, like filing a claim or appealing a coverage decision. How do i file a claim? Free medicare publications medicare & you handbook;
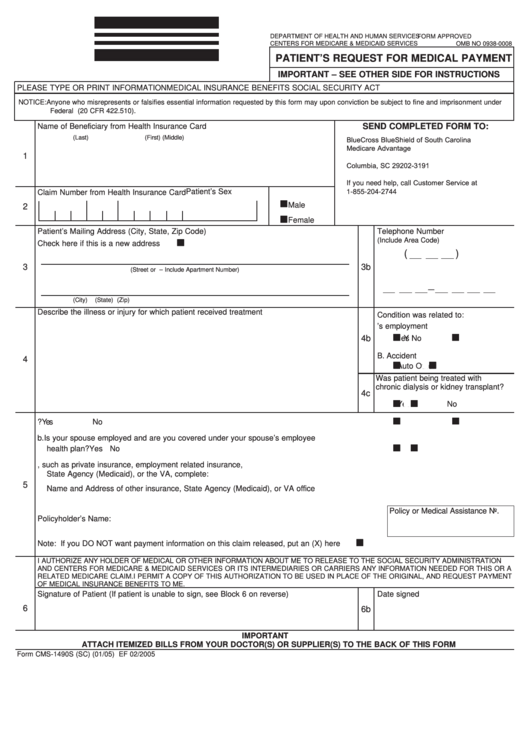
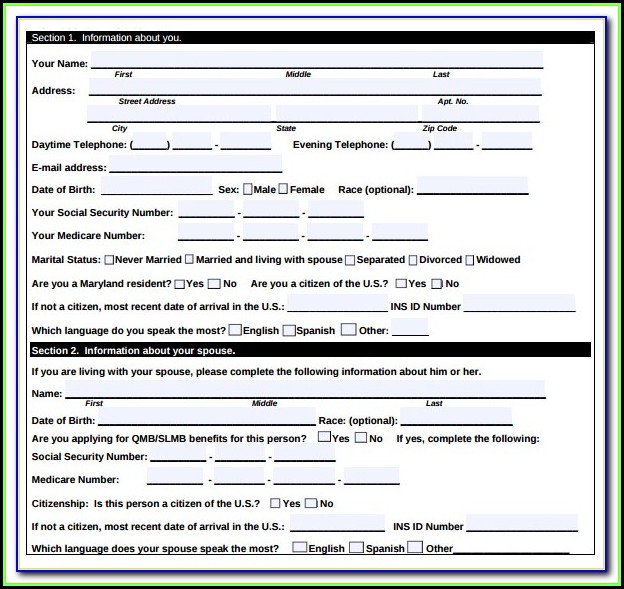
The provided link below includes the form and all the applicable instructions. Web name of beneficiary from health insurance card (last)(first) (middle) claim number from health insurance card patient’s sex male female send completed form to: Enclosed is the form, instructions for completing it, and where to return. Mail your completed claim form to the medicare carrier responsible for processing your claim. Web patient's request for medical payment. Web if you need to file your own medicare claim, you’ll need to fill out a patient request for medical payment form, the 1490s. Filing a claim when you get services and/or supplies (if your provider doesn’t file it). Web download claims with medicare's blue button; Web cms forms list. (2) mail the completed form and itemized bills to the correct medicare administrative contractor as indicated on.
Please read all instructions prior to submitting a claim to medicare. The provided link below includes the form and all the applicable instructions. What do i submit with the claim? Web the provided link below includes the form and all the applicable instructions. Free medicare publications medicare & you handbook; This particular form is known as the patient’s request for medical payment form. Get all forms in alternate formats. Enclosed is the form, instructions for completing it, and where to return the form for processing. If the beneficiary has any questions about their claim or how to complete the claim form, they must call 1. Send the form to the company that processes your medicare claims.
Form Cms1490s (Sc) Patient'S Request For Medical Payment printable
If the beneficiary has any questions about their claim or how to complete the claim form, they must call 1. (2) mail the completed form and itemized bills to the correct medicare administrative contractor as indicated on. Mail you get about medicare; Web download claims with medicare's blue button; Web patient's request for medical payment.
Medicare Claim Form Cms 1490s Form Resume Examples djVaBnG2Jk
Patient’s request for medical payment) is used for collecting the personal information of a patient who needs to request payment for the furnished medical procedures. Get all forms in alternate formats. Web cms forms list. Get a fillable form 1490s template online. Forms get medicare forms for different situations, like filing a claim or appealing a coverage decision.
What Is The 1490s Medicare Form
Web patient's request for medical payment. Mail your completed claim form to the medicare contractor responsible for processing your claim. Forms get medicare forms for different situations, like filing a claim or appealing a coverage decision. Send the form to the company that processes your medicare claims. Please read all instructions prior to submitting a claim to medicare.

Medicare Claim Form Cms 1490s Form Resume Examples djVaBnG2Jk
What do i submit with the claim? Forms get medicare forms for different situations, like filing a claim or appealing a coverage decision. Please retain a copy of the cms 1490s claim form and. Mail your completed claim form to the medicare carrier responsible for processing your claim. Complete and sign it in seconds from your desktop or mobile device,.
Medicare Form 1490s Instructions Form Resume Examples Wk9yGWvV3D
The provided link below includes the form and all the applicable instructions. Patient’s request for medical payment) is used for collecting the personal information of a patient who needs to request payment for the furnished medical procedures. Web if you need to file your own medicare claim, you’ll need to fill out a patient request for medical payment form, the.
Medicare Claim Form Cms 1490s Form Resume Examples djVaBnG2Jk
Get a fillable form 1490s template online. The following provides access and/or information for many cms forms. Web the claim and supporting documentation must be sent to the medicare administrative contractor (mac) responsible for the state in which you received the services. Web name of beneficiary from health insurance card (last)(first) (middle) claim number from health insurance card patient’s sex.
Medicare Form 1490s Instructions Form Resume Examples Wk9yGWvV3D
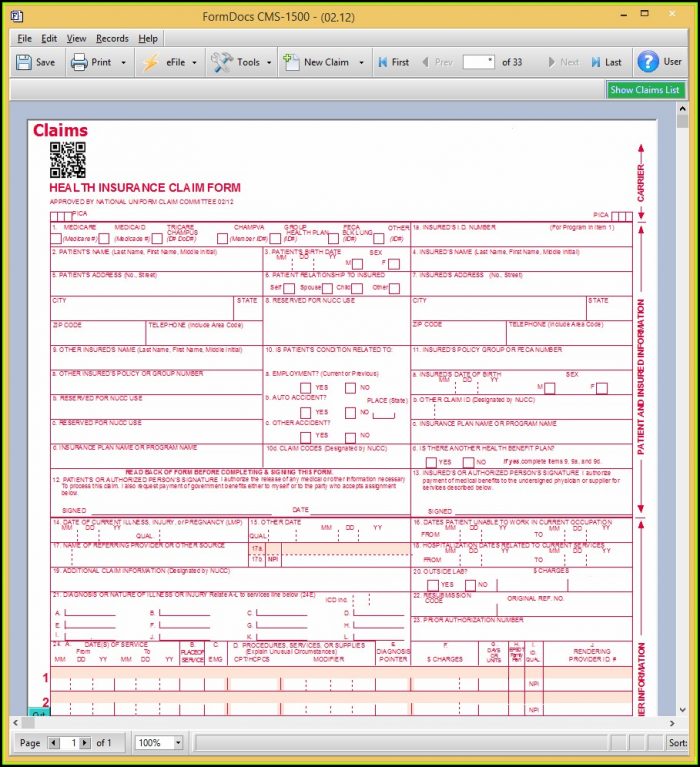
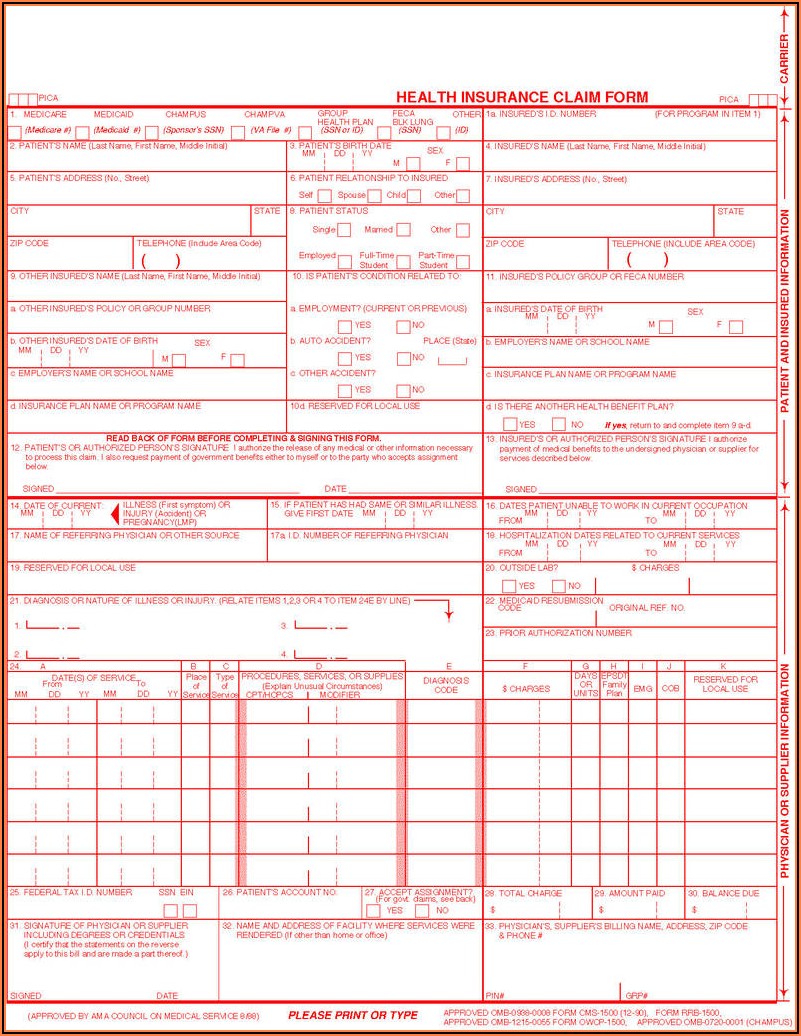
• name, medicare number, and address • description of the service or medical item • itemized bill containing the following information: Get all forms in alternate formats. Medicare can’t pay its share if the submission doesn’t happen within 12 months. Mail your completed claim form to the medicare contractor responsible for processing your claim. Web download claims with medicare's blue.

Medicare Claim Form Cms 1490s Form Resume Examples ygKz4RV8P9
Enclosed is the form, instructions for completing it, and where to return. • name, medicare number, and address • description of the service or medical item • itemized bill containing the following information: How do i file a claim? Web name of beneficiary from health insurance card (last)(first) (middle) claim number from health insurance card patient’s sex male female send.

Medicare Claim Form Cms 1490s Form Resume Examples djVaBnG2Jk
Filing a claim when you get services and/or supplies (if your provider doesn’t file it). The following provides access and/or information for many cms forms. The provided link below includes the form and all the applicable instructions. Mail you get about medicare; Date of service place of service description of service charge for service
Medicare Claim Form Cms 1490s Form Resume Examples djVaBnG2Jk
Web name of beneficiary from health insurance card (last)(first) (middle) claim number from health insurance card patient’s sex male female send completed form to: Web get forms to file a claim, set up recurring premium payments, and more. Mail your completed claim form to the medicare contractor responsible for processing your claim. How do i file a claim? Web a.
Web If You Need To File Your Own Medicare Claim, You’ll Need To Fill Out A Patient Request For Medical Payment Form, The 1490S.
Web the claim and supporting documentation must be sent to the medicare administrative contractor (mac) responsible for the state in which you received the services. Web cms forms list. Web patient's request for medical payment. Enclosed is the form, instructions for completing it, and where to return.
Mail Your Completed Claim Form To The Medicare Contractor Responsible For Processing Your Claim.
Web download claims with medicare's blue button; Web get forms to file a claim, set up recurring premium payments, and more. Mail your completed claim form to the medicare carrier responsible for processing your claim. This particular form is known as the patient’s request for medical payment form.
Find Forms Publications Read, Print, Or Order Free Medicare Publications In A Variety Of Formats.
Send the form to the company that processes your medicare claims. Please retain a copy of the cms 1490s claim form and. How do i file a claim? What do i submit with the claim?
Web A Cms 1490S Form Will Be Used By The Centers For Medicare And Medicaid Services.
Web name of beneficiary from health insurance card (last)(first) (middle) claim number from health insurance card patient’s sex male female send completed form to: Web medicare may pay you directly when you complete this form and attach an itemized bill from your doctor or supplier. Web the provided link below includes the form and all the applicable instructions. Enclosed is the form, instructions for completing it, and where to return the form for processing.