Hipaa Right Of Access Form For Family Member Friend
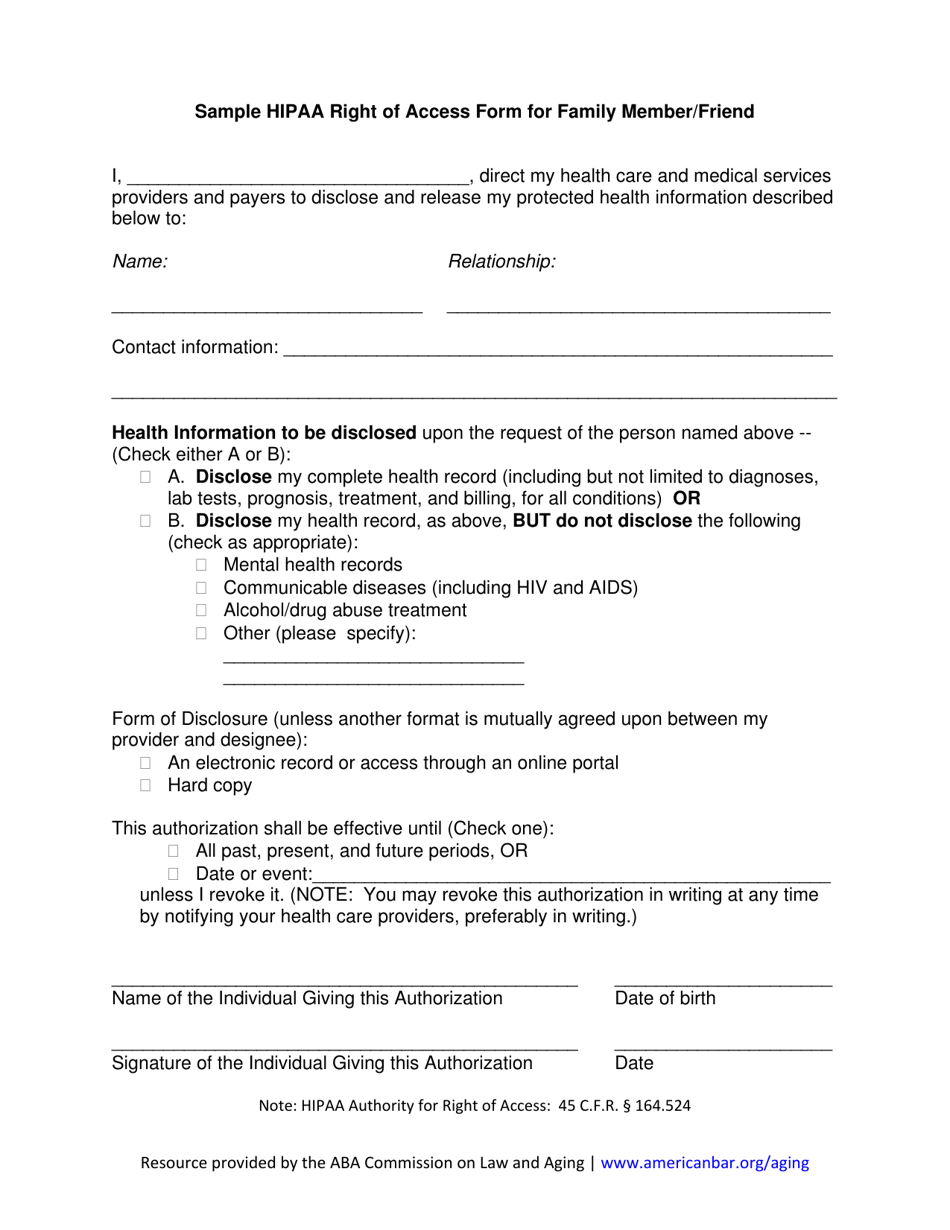
Hipaa Right Of Access Form For Family Member Friend - Form of disclosure (unless another format is mutually agreed upon between my provider and designee): Web hipaa right of access form for family member/friend note: Specifically, a covered entity is permitted to. Web right of access form for family member/friend. This form allows you to direct health care providers and payers to disclose and release protected health. Web share your rights under hipaa this guidance remains in effect only to the extent that it is consistent with the court’s order in ciox health, llc v. I, first name * last name * , direct champion health associates, llc to disclose and release my protected health. However, if you don’t object, a health. Indeed, a personal representative generally has the. Authorizations (30) business associates (41) compliance dates (2) covered essences (14) decedents (9) disclosures for law.
Web hipaa right of access form for family member / friend i, __________________________________, authorize christian healthcare centers to. Indeed, a personal representative generally has the. Web page 3 of 5 communicating with a patient’s family, friends, or others involved in the patient’s care 5. Web outside of the hipaa right of access, other provisions in the privacy rule address disclosures to family members. Hipaa right of access form for family member/friend i, _________________________________, direct my health care and medical services. This form allows you to direct health care providers and payers to disclose and release protected health. Ad sample hipaa right of access form & more fillable forms, register and subscribe now! An electronic record or access through an online portal. Try it for free now! Web the hipaa privacy rule at 45 cfr 164.510(b) specifically permits covered entities to share information that is directly relevant to the involvement of a spouse, family members,.
Web sample hipaa right of access form for family member/friends. Web the hipaa privacy rule at 45 cfr 164.510(b) specifically permits covered entities to share information that is directly relevant to the involvement of a spouse, family members,. Easily customize your hipaa authorization form. If a patient’s family member, friend, or other person involved in the. The hipaa privacy rule at 45 cfr 164.510 (b) specifically permits covered entities to share information that is directly relevant to the involvement of a spouse, family. Web disclosures to family press friends ; § 164.524 health information greene county health care is. Hipaa right of access form for family member/friend i, _________________________________, direct my health care and medical services. Specifically, a covered entity is permitted to. Web outside of the hipaa right of access, other provisions in the privacy rule address disclosures to family members.

Fierce Healthcare Industry Voices Turn of the Tides Patients
Hipaa authority for right of access: Hipaa right of access form for family member/friend i, _________________________________, direct my health care and medical services. Web page 3 of 5 communicating with a patient’s family, friends, or others involved in the patient’s care 5. Web hipaa allows healthcare providers to disclose protected health information to the patient’s personal representative; Web share your.
HIPAA Right of Access Form for Family Member/Friend Download Printable
I, first name * last name * , direct champion health associates, llc to disclose and release my protected health. Web sample hipaa right of access form for family member/friends. Web hipaa allows healthcare providers to disclose protected health information to the patient’s personal representative; Hipaa authority for right of access: Indeed, a personal representative generally has the.

HIPAA Right of Access Myths HIPAA Secure Now!
Web watch newsmax live for the latest news and analysis on today's top stories, right here on facebook. Ad sample hipaa right of access form & more fillable forms, register and subscribe now! If a patient’s family member, friend, or other person involved in the. Web hipaa right of access form for family member/friend i, _____, direct my health care.
What You Need to Know About HIPAA Patient Right of Access Laws Abyde
Web hipaa right of access form for family member/friend. Easily customize your hipaa authorization form. Web disclosures to family press friends ; Web hipaa right of access form for family member/friend i, ________________________________, direct my health care and medical services. I, first name * last name * , direct champion health associates, llc to disclose and release my protected health.

HIPAA Right of access costs two more providers under the HIPAA privacy
Hipaa right of access form for family member/friend i, _________________________________, direct my health care and medical services. Ad answer simple questions to make a hipaa authorization form on any device in minutes. Specifically, a covered entity is permitted to. Web hipaa right of access form for family member/friend i, ________________________________, direct my health care and medical services. Try it for.

HIPAA Right of Access HIPAA Secure Now!
Hipaa right of access form for family member/friend i, _________________________________, direct my health care and medical services. I, first name * last name * , direct champion health associates, llc to disclose and release my protected health. Web hipaa right of access form for family member/friend i, direct my health care and medical services providers and payers to disclose and.
What Is HIPAA And How Does It Work? Managed IT Services and Cyber
Web hipaa right of access form for family member/friend i, _____, direct my health care and medical services providers and payers to disclose and release my protected health. Web hipaa right of access form for family member/friend. Specifically, a covered entity is permitted to. Web sample hipaa right of access form for family member/friends. Web the hipaa privacy rule at.

HIPAA Violation Fines and Penalties What Are They in 2020? Your Key
Upload, modify or create forms. The hipaa privacy rule at 45 cfr 164.510 (b) specifically permits covered entities to share information that is directly relevant to the involvement of a spouse, family. Web hipaa right of access form for family member/friend i, ________________________________, direct my health care and medical services. Try it for free now! This form allows you to.
OCR Announces the 11th HIPAA Right of Access Settlement Abyde
Web hipaa right of access form for family member/friend. Upload, modify or create forms. Web hipaa right of access form for family member / friend i, __________________________________, authorize christian healthcare centers to. If a patient’s family member, friend, or other person involved in the. Hipaa right of access form for family member/friend i, _________________________________, direct my health care and medical.
OCR Settles Cases in HIPAA Right of Access Initiative HealthLeaders Media
Web hipaa right of access form for family member/friend i, _____, direct my health care and medical services providers and payers to disclose and release my protected health. § 164.524 health information greene county health care is. Hipaa right of access form for family member/friend i, _________________________________, direct my health care and medical services. Web hipaa right of access form.
Web Hipaa Right Of Access Form For Family Member/Friend.
Web hipaa right of access form for family member/friend i, direct my health care and medical services providers and payers to disclose and release my protected health. Web disclosures to family press friends ; § 164.524 health information greene county health care is. Web hipaa right of access form for family member/friend i, ________________________________, direct my health care and medical services.
This Form Allows You To Direct Health Care Providers And Payers To Disclose And Release Protected Health.
Hipaa requires health care providers to protect the privacy of your health information. Indeed, a personal representative generally has the. Web hipaa right of access form for family member / friend i, __________________________________, authorize christian healthcare centers to. Upload, modify or create forms.
Try It For Free Now!
Web hipaa right of access form for family member/friend i, _____, direct image eye care to disclose and. I, first name * last name * , direct champion health associates, llc to disclose and release my protected health. Web hipaa right of access form for family member/friend. If a patient’s family member, friend, or other person involved in the.
Easily Customize Your Hipaa Authorization Form.
Web watch newsmax live for the latest news and analysis on today's top stories, right here on facebook. Form of disclosure (unless another format is mutually agreed upon between my provider and designee): Ad sample hipaa right of access form & more fillable forms, register and subscribe now! However, if you don’t object, a health.