Cigna Appeals Form
Cigna Appeals Form - Do not include a copy of a claim that was previously processed. Provide additional information to support the description of the dispute. Web instructions please complete the below form. We may be able to resolve your issue quickly outside of the formal appeal process. Learn about appeals for medicare plans. Web to initiate a review of a health care provider's termination, submit the following information in writing within 30 calendar days of the date of the health care provider's termination notice. Be specific when completing the description of dispute and expected outcome. Web appeals forms billing dispute resolution form [pdf] billing dispute external review form [pdf] appeal request form [pdf] provider payment review [pdf] california appeal request form [pdf] new jersey appeal request form [pdf] medicare provider appeal form medicare customer appeal form How to request an appeal if you have a plan through your employer If only submitting a letter, please specify in the letter this is a health care professional appeal.
Fields with an asterisk ( * ) are required. How to request an appeal if you have a plan through your employer Web to initiate a review of a health care provider's termination, submit the following information in writing within 30 calendar days of the date of the health care provider's termination notice. Learn about appeals for medicare plans. Check the box that most closely describes your appeal or reconsideration reason. We may be able to resolve your issue quickly outside of the formal appeal process. A completed health care provider termination appeal letter indicating the reason for the appeal. Be specific when completing the description of dispute and expected outcome. If only submitting a letter, please specify in the letter this is a health care professional appeal. Web instructions please complete the below form.
Web to initiate a review of a health care provider's termination, submit the following information in writing within 30 calendar days of the date of the health care provider's termination notice. Learn about appeals for medicare plans. How to request an appeal if you have a plan through your employer Do not include a copy of a claim that was previously processed. Or, if you're a mycigna user, log in to mycigna and go to the forms center. Be sure to include any supporting documentation, as indicated below. Web this completed form and/or an appeal letter requesting an appeal review and indicating the reason(s) why you believe the claim payment is incorrect and should be changed. Provide additional information to support the description of the dispute. We may be able to resolve your issue quickly outside of the formal appeal process. Check the box that most closely describes your appeal or reconsideration reason.
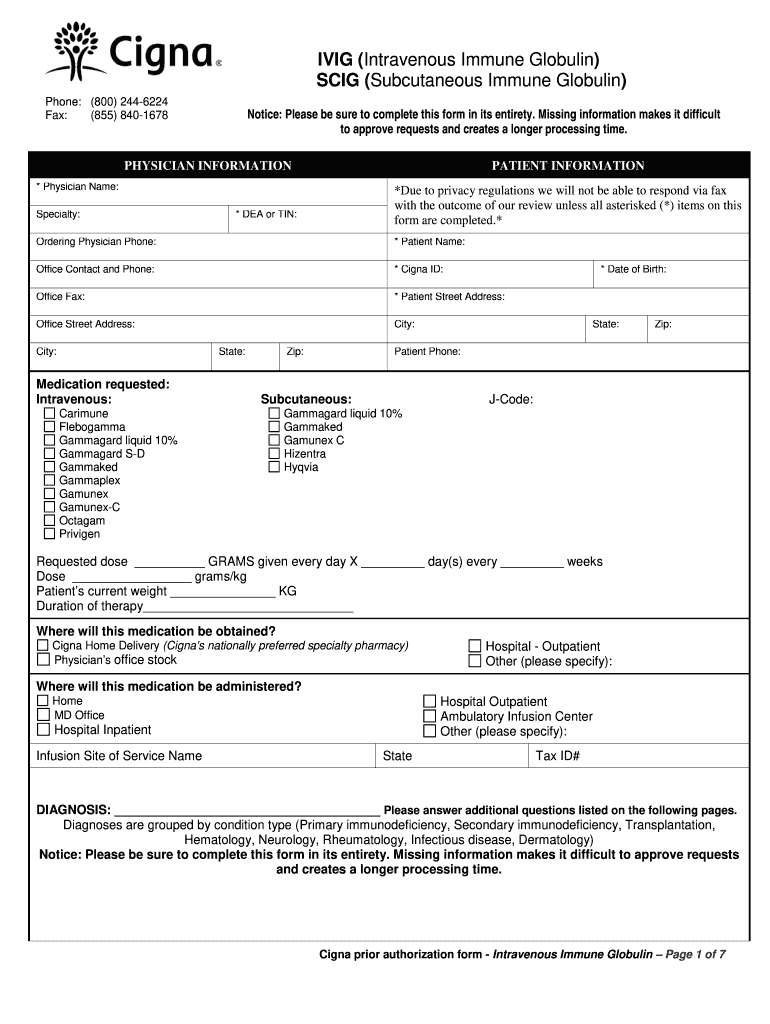
Cigna Ivig Prior Authorization Form Fill Out and Sign Printable PDF
Web to initiate a review of a health care provider's termination, submit the following information in writing within 30 calendar days of the date of the health care provider's termination notice. Be sure to include any supporting documentation, as indicated below. Check the box that most closely describes your appeal or reconsideration reason. Fields with an asterisk ( * ).
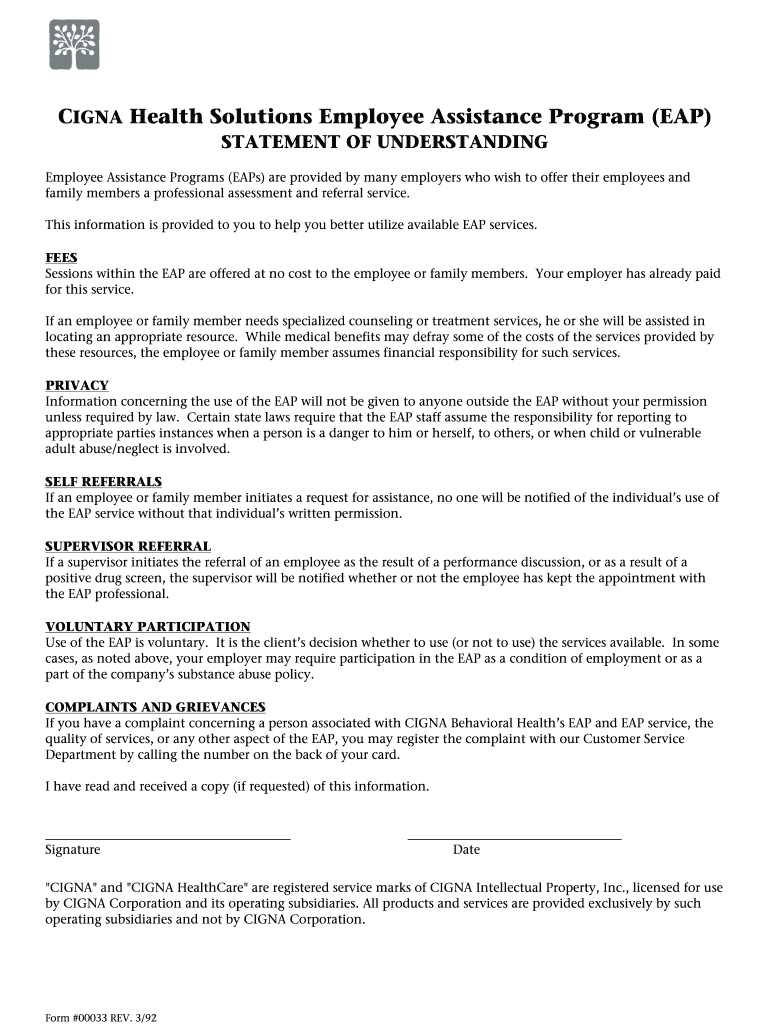
Cigna Eap Form Fill Out and Sign Printable PDF Template signNow
We may be able to resolve your issue quickly outside of the formal appeal process. Web instructions please complete the below form. If only submitting a letter, please specify in the letter this is a health care professional appeal. Be sure to include any supporting documentation, as indicated below. Do not include a copy of a claim that was previously.

Cigna Employee Assistance Program
Or, if you're a mycigna user, log in to mycigna and go to the forms center. Web instructions please complete the below form. Learn about appeals for medicare plans. Web to file an appeal or grievance: Do not include a copy of a claim that was previously processed.
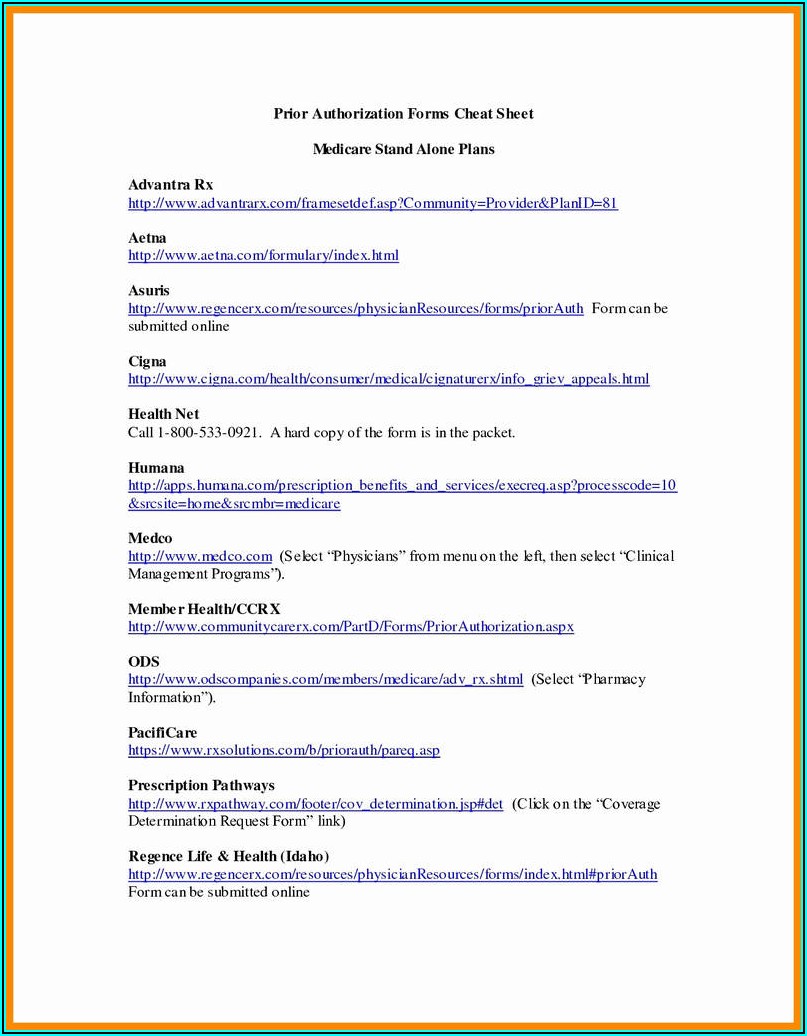
Cigna Medicare Part D Medication Prior Authorization Form Form
Do not include a copy of a claim that was previously processed. Check the box that most closely describes your appeal or reconsideration reason. Web instructions please complete the below form. Web to file an appeal or grievance: If submitting a letter, please include all information requested on this form.

Cigna Claim Form Payments Cigna
If only submitting a letter, please specify in the letter this is a health care professional appeal. We may be able to resolve your issue quickly outside of the formal appeal process. Web to initiate a review of a health care provider's termination, submit the following information in writing within 30 calendar days of the date of the health care.
Cigna Ranks Safecare's Physicians as Top Performers Safecare Medical
Provide additional information to support the description of the dispute. Web instructions please complete the below form. How to request an appeal if you have a plan through your employer Web appeals and reconsideration request form complete the top section of this form completely and legibly. Requests received without required information cannot be processed.
Things to Know about Cigna Home Delivery Pharmacy
Web instructions please complete the below form. Web appeals forms billing dispute resolution form [pdf] billing dispute external review form [pdf] appeal request form [pdf] provider payment review [pdf] california appeal request form [pdf] new jersey appeal request form [pdf] medicare provider appeal form medicare customer appeal form If submitting a letter, please include all information requested on this form..
Cigna Appeal Form Fill Out and Sign Printable PDF Template signNow
Fields with an asterisk ( * ) are required. How to request an appeal if you have a plan through your employer Web appeals forms billing dispute resolution form [pdf] billing dispute external review form [pdf] appeal request form [pdf] provider payment review [pdf] california appeal request form [pdf] new jersey appeal request form [pdf] medicare provider appeal form medicare.
Fillable Form 61211 Prescription Drug Prior Authorization Request
Be sure to include any supporting documentation, as indicated below. Check the box that most closely describes your appeal or reconsideration reason. Be specific when completing the description of dispute and expected outcome. Provide additional information to support the description of the dispute. Do not include a copy of a claim that was previously processed.
Medical Claim Form Cigna Nal Printable Cms United Healthcare with Med
If only submitting a letter, please specify in the letter this is a health care professional appeal. Do not include a copy of a claim that was previously processed. Or, if you're a mycigna user, log in to mycigna and go to the forms center. Web this completed form and/or an appeal letter requesting an appeal review and indicating the.
Web To File An Appeal Or Grievance:
Web this completed form and/or an appeal letter requesting an appeal review and indicating the reason(s) why you believe the claim payment is incorrect and should be changed. If only submitting a letter, please specify in the letter this is a health care professional appeal. Requests received without required information cannot be processed. A completed health care provider termination appeal letter indicating the reason for the appeal.
Web Appeals Forms Billing Dispute Resolution Form [Pdf] Billing Dispute External Review Form [Pdf] Appeal Request Form [Pdf] Provider Payment Review [Pdf] California Appeal Request Form [Pdf] New Jersey Appeal Request Form [Pdf] Medicare Provider Appeal Form Medicare Customer Appeal Form
Provide additional information to support the description of the dispute. How to request an appeal if you have a plan through your employer Be specific when completing the description of dispute and expected outcome. If submitting a letter, please include all information requested on this form.
Web To Initiate A Review Of A Health Care Provider's Termination, Submit The Following Information In Writing Within 30 Calendar Days Of The Date Of The Health Care Provider's Termination Notice.
Or, if you're a mycigna user, log in to mycigna and go to the forms center. Web appeals and reconsideration request form complete the top section of this form completely and legibly. Learn about appeals for medicare plans. Web instructions please complete the below form.
Do Not Include A Copy Of A Claim That Was Previously Processed.
We may be able to resolve your issue quickly outside of the formal appeal process. Fields with an asterisk ( * ) are required. Be sure to include any supporting documentation, as indicated below. Check the box that most closely describes your appeal or reconsideration reason.