Bcbs Tx Appeal Form
Bcbs Tx Appeal Form - Provider compliance challenges with prenatal appointment availability. Mail or fax it to us using the address or fax number listed at the top of the form. Web please complete one form per member to request an appeal of an adjudicated/paid claim. Fields with an asterisk (*) are required. Web fill out a health plan appeal request form. You may file an appeal in writing by sending a letter or fax: If coverage or payment for an item or medical service is denied that you think should be covered. Just call the phone number printed on your bcbstx id card. Please fill out this form and attach any papers that support this request. Read the hhsc how to submit a complaint flyer to find out how to file a complaint.
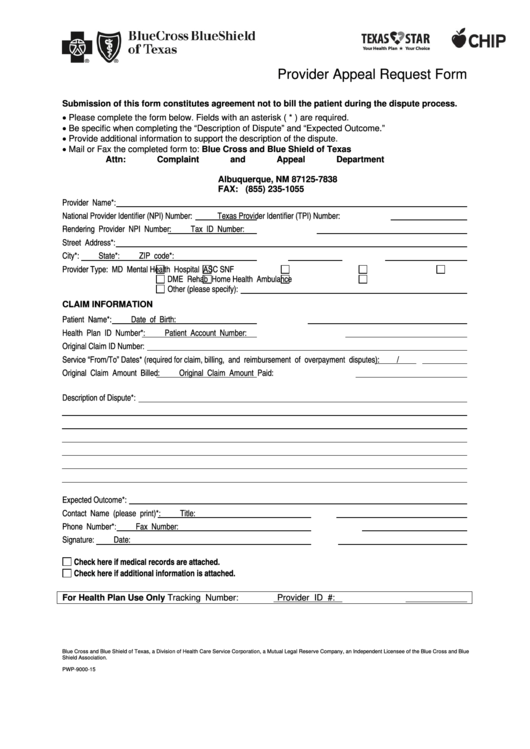
Read the hhsc how to submit a complaint flyer to find out how to file a complaint. You may also file an appeal by phone. Please fill out this form and attach any papers that support this request. Blue cross and blue shield of texas (bcbstx) c/o complaints and appeals department. If coverage or payment for an item or medical service is denied that you think should be covered. Be specific when completing the “description of appeal” and “expected outcome.” provide additional information to support the description of the appeal. Be specific when completing the “description of appeal” and “expected outcome.” please provider all. You can ask for an appeal: Blue cross and blue shield of texas Access and download these helpful bcbstx health care provider forms.
Box 663099 dallas, tx 75266. Web fill out a health plan appeal request form. Web member appeal request form. Appeals must be submitted within 120 days of the remittance date. This form must be placed on top of the correspondence you are. Fields with an asterisk (*) are required. Blue cross and blue shield of texas Blue cross and blue shield of texas (bcbstx) c/o complaints and appeals department. Web please complete one form per member to request an appeal of an adjudicated/paid claim. Please attach supporting documentation to facilitate your review, for example the operative report, or medical records, etc.
BCBSTX Offers Special Enrollment Options
Mail or fax it to us using the address or fax number listed at the top of the form. Web please complete one form per member to request an appeal of an adjudicated/paid claim. Blue cross and blue shield of texas Appeals must be submitted within 120 days of the remittance date. Read the hhsc how to submit a complaint.

pare And Contrast The Various Types Governme
Just call the phone number printed on your bcbstx id card. This form must be placed on top of the correspondence you are. Read the hhsc how to submit a complaint flyer to find out how to file a complaint. Web request for claim appeal/reconsideration review form do not attach claim forms unless changes have been made from the original.

KS BCBS 37024 20192022 Fill and Sign Printable Template Online US
Provider compliance challenges with prenatal appointment availability. You may file an appeal in writing by sending a letter or fax: 711), monday through friday, 8 a.m. Just call the phone number printed on your bcbstx id card. Box 663099 dallas, tx 75266.
Bluecross Blueshield Of Texas Provider Appeal Request Form printable
Web please complete one form per member to request an appeal of an adjudicated/paid claim. Fields with an asterisk (*) are required. Blue cross and blue shield of texas You may file an appeal in writing by sending a letter or fax: Rate enhancement for attendant compensation form.

TN BCBS 17PED153727 20172021 Fill and Sign Printable Template Online
Please attach supporting documentation to facilitate your review, for example the operative report, or medical records, etc. Fields with an asterisk (*) are required. 711), monday through friday, 8 a.m. Provider compliance challenges with prenatal appointment availability. Read the hhsc how to submit a complaint flyer to find out how to file a complaint.

Liberty Mutual Network
Web dme request for claim status form. To 5 p.m., central time. Web request for claim appeal/reconsideration review form do not attach claim forms unless changes have been made from the original claim that was submitted. You can ask for an appeal: You may also file an appeal by phone.

Bcbs Federal Provider Appeal form Inspirational Pdf the Notice
Read the hhsc how to submit a complaint flyer to find out how to file a complaint. Provider compliance challenges with prenatal appointment availability. Web please complete one form per member to request an appeal of an adjudicated/paid claim. Web blue cross blue shield of texas is committed to giving health care providers with the support and assistance they need..
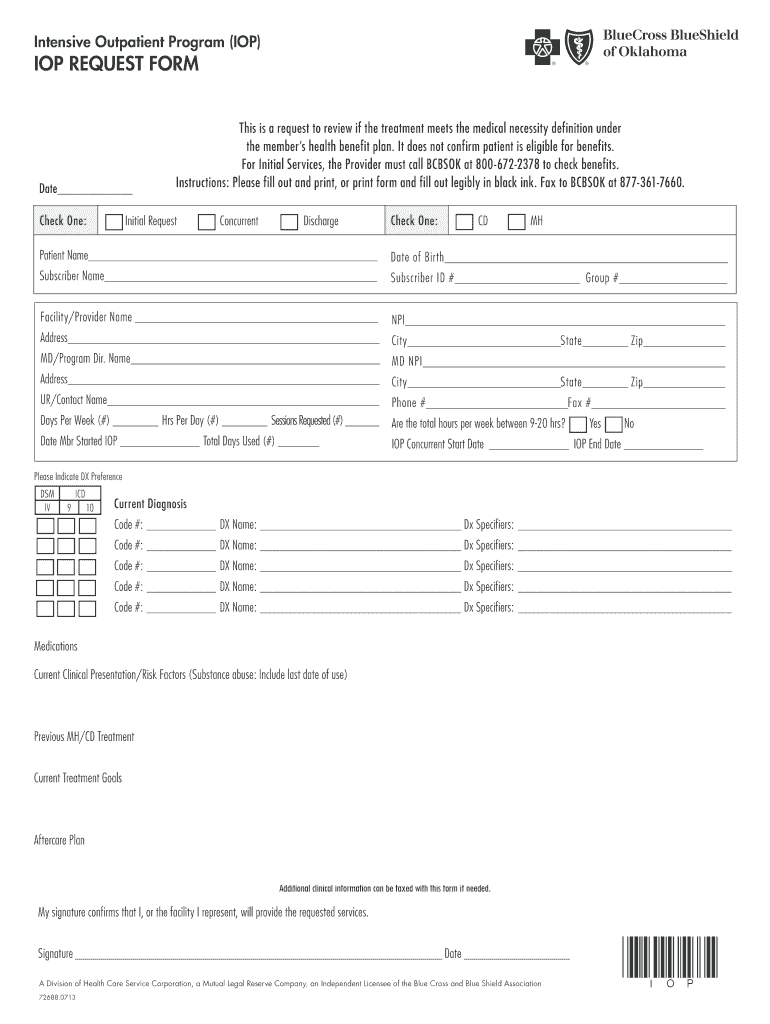
bcbs iop request form Fill out & sign online DocHub
Web member appeal request form. Fields with an asterisk (*) are required. Web blue cross blue shield of texas is committed to giving health care providers with the support and assistance they need. Blue cross and blue shield of texas (bcbstx) c/o complaints and appeals department. To 5 p.m., central time.
BCBSTX Home Blue Cross And Blue Shield Of Texas Fill Out and Sign
Blue cross medicare advantage c/o appeals p.o. Web dme request for claim status form. This form must be placed on top of the correspondence you are. If coverage or payment for an item or medical service is denied that you think should be covered. Blue cross and blue shield of texas
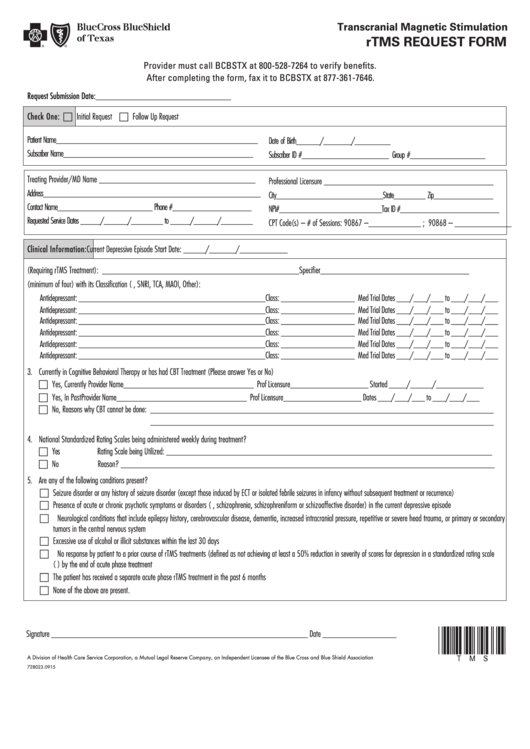
Fillable Repetitive Transcranial Stimulation (Rtms) Request
Please attach supporting documentation to facilitate your review, for example the operative report, or medical records, etc. Blue cross and blue shield of texas (bcbstx) c/o complaints and appeals department. Appeals must be submitted within 120 days of the remittance date. Blue cross and blue shield of texas Web blue cross blue shield of texas is committed to giving health.
Mail Or Fax It To Us Using The Address Or Fax Number Listed At The Top Of The Form.
Please attach supporting documentation to facilitate your review, for example the operative report, or medical records, etc. Blue cross and blue shield of texas (bcbstx) c/o complaints and appeals department. Web fill out a health plan appeal request form. To 5 p.m., central time.
Fields With An Asterisk (*) Are Required.
Please fill out this form and attach any papers that support this request. Provider compliance challenges with prenatal appointment availability. Web blue cross blue shield of texas is committed to giving health care providers with the support and assistance they need. You can ask for an appeal:
711), Monday Through Friday, 8 A.m.
If coverage or payment for an item or medical service is denied that you think should be covered. Fields with an asterisk (*) are required. Web please complete one form per member to request an appeal of an adjudicated/paid claim. This form must be placed on top of the correspondence you are.
Be Specific When Completing The “Description Of Appeal” And “Expected Outcome.” Provide Additional Information To Support The Description Of The Appeal.
Read the hhsc how to submit a complaint flyer to find out how to file a complaint. You may file an appeal in writing by sending a letter or fax: Just call the phone number printed on your bcbstx id card. Blue cross medicare advantage c/o appeals p.o.