Ambetter Claim Form
Ambetter Claim Form - Web member reimbursement medical claim form (please complete one form per family member per provider) instructions 1.you will need your health care provider to. Web use this form as part of the ambetter from coordinated care request for reconsideration and claim dispute process. Web ambetter does not supply claim forms to providers. Your ambetter online member account puts you in. Maintaining accreditation is ambetter’s long. Envolve pharmacy solutions | 5 river park place east, suite 210 | fresno,. Submitting a claim or claim reconsideration/dispute. Box 5010 • farmington, mo 63640. The claim dispute form must be completed in its. Web prescription claim reimbursement form for claim reimbursement, complete and mail to:
Web a claim dispute/claim appeal must be submitted on this claim dispute/appeal form, which can also be found on our website. No surprises act open negotiation form (pdf) quality. Submitting a claim or claim reconsideration/dispute. Web claims and claim payment. Web please submit this form and all documentation to: Use your zip code to find your personal plan. Level of dispute (please check): Web 2022 provider and billing manual (pdf) 2021 provider and billing manual (pdf) quick reference guide (pdf) prior authorization guide (pdf) secure portal (pdf) payspan. Your ambetter online member account puts you in. All paper claim forms must be typed with.
Web a claim dispute/claim appeal must be submitted on this claim dispute/appeal form, which can also be found on our website. Level of dispute (please check): Web use this form as part of the ambetter from superior healthplanrequest for reconsideration and claim dispute process. Web please submit this form and all documentation to: Envolve pharmacy solutions | 5 river park place east, suite 210 | fresno,. Web use this form as part of the ambetter from coordinated care request for reconsideration and claim dispute process. The claim dispute form must be completed in its. Web “corrected claim” process in the provider manual. See coverage in your area; All paper claim forms must be typed with.

Ambetter Member Reimbursement Medical Claim Form
Box 5010 • farmington, mo 63640. Maintaining accreditation is ambetter’s long. Web prescription claim reimbursement form for claim reimbursement, complete and mail to: Web use this form as part of the ambetter from coordinated care request for reconsideration and claim dispute process. No surprises act open negotiation form (pdf) quality.
Who Accepts Ambetter Health Insurance insurance
Web 2022 provider and billing manual (pdf) 2021 provider and billing manual (pdf) quick reference guide (pdf) prior authorization guide (pdf) secure portal (pdf) payspan. Web a claim dispute/claim appeal must be submitted on this claim dispute/appeal form, which can also be found on our website. Providers should purchase these from a supplier of their choice. See coverage in your.

Who Accepts Ambetter Health Insurance insurance
Web please submit this form and all documentation to: The claim dispute form must be completed in its. Web use this form as part of the ambetter from coordinated care request for reconsideration and claim dispute process. Box 5010 • farmington, mo 63640. Web “corrected claim” process in the provider manual.
What is Ambetter? YouTube
All paper claim forms must be typed with. Use your zip code to find your personal plan. Box 5010 • farmington, mo 63640. Please do not include this form with a corrected claim. Level of dispute (please check):
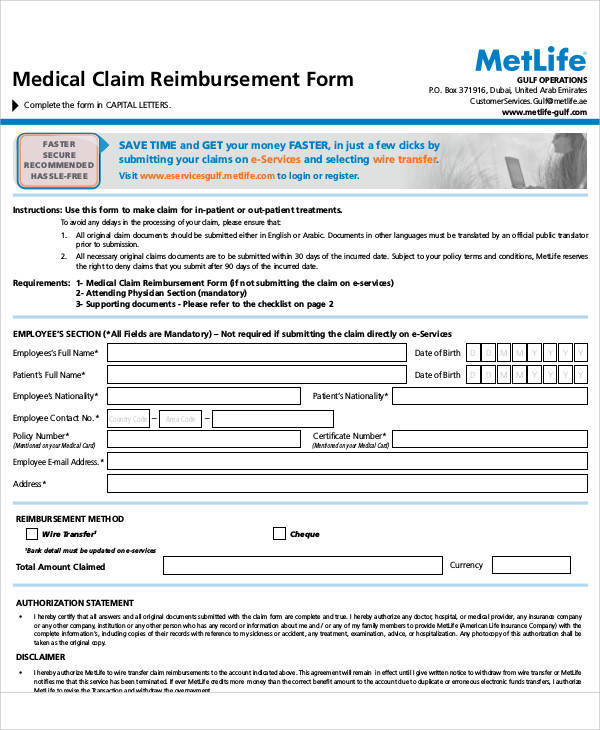
Aetna Reimbursement Claim Form alacarddesign
Web claims and claim payment. Web “corrected claim” process in the provider manual. Use your zip code to find your personal plan. All fields are required information a request for. Claim dispute form (pdf) billing and coding;

Ambetter Health Insurance Ambetter Reviews and Complaints 2020
Providers should purchase these from a supplier of their choice. Web 2022 provider and billing manual (pdf) 2021 provider and billing manual (pdf) quick reference guide (pdf) prior authorization guide (pdf) secure portal (pdf) payspan. All fields are required information a request for. Claim dispute form (pdf) billing and coding; Your ambetter online member account puts you in.
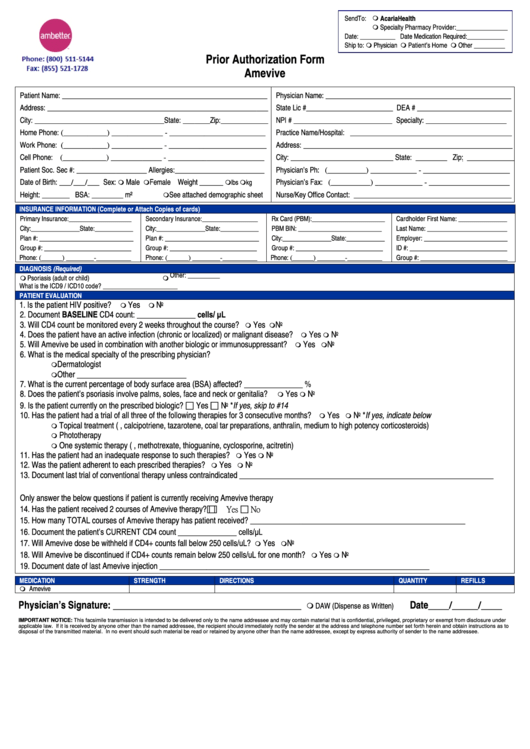
Ambetter Prior Authorization Form Amevive printable pdf download
Submitting a claim or claim reconsideration/dispute. Box 5010 • farmington, mo 63640. Please do not include this form with a corrected claim. Web member reimbursement medical claim form (please complete one form per family member per provider) instructions 1.you will need your health care provider to. Level of dispute (please check):
FREE 50+ Sample Claim Forms in PDF MS Word
Envolve pharmacy solutions | 5 river park place east, suite 210 | fresno,. All fields are required information a request for. Level of dispute (please check): Claim dispute form (pdf) billing and coding; All paper claim forms must be typed with.

Envolve Vision Newsletter Volume 6 Issue 3 National English
Web use this form as part of the ambetter from superior healthplanrequest for reconsideration and claim dispute process. Please do not include this form with a corrected claim. All fields are required information provider name provider. Submitting a claim or claim reconsideration/dispute. Web 2022 provider and billing manual (pdf) 2021 provider and billing manual (pdf) quick reference guide (pdf) prior.

Ambetter Health Insurance Coverage For Drug Rehab
Web “corrected claim” process in the provider manual. Web a claim dispute/claim appeal must be submitted on this claim dispute/appeal form, which can also be found on our website. All paper claim forms must be typed with. Web ambetter provider claims & payments faq quick links (questions are grouped into the following categories): All fields are required information a request.
Web Use This Form As Part Of The Ambetter From Superior Healthplanrequest For Reconsideration And Claim Dispute Process.
Web there, you can find information about your ambetter coverage, access options for care and much more — all in one place. All fields are required information provider name provider. Your ambetter online member account puts you in. Level of dispute (please check):
Web “Corrected Claim” Process In The Provider Manual.
Web ambetter provider claims & payments faq quick links (questions are grouped into the following categories): Web please submit this form and all documentation to: Use your zip code to find your personal plan. Web ambetter does not supply claim forms to providers.
Web Prescription Claim Reimbursement Form For Claim Reimbursement, Complete And Mail To:
Web a claim dispute/claim appeal must be submitted on this claim dispute/appeal form, which can also be found on our website. Please do not include this form with a corrected claim. Providers should purchase these from a supplier of their choice. Web 2022 provider and billing manual (pdf) 2021 provider and billing manual (pdf) quick reference guide (pdf) prior authorization guide (pdf) secure portal (pdf) payspan.
Envolve Pharmacy Solutions | 5 River Park Place East, Suite 210 | Fresno,.
Web member reimbursement medical claim form (please complete one form per family member per provider) instructions 1.you will need your health care provider to. Web use this form as part of the ambetter from coordinated care request for reconsideration and claim dispute process. The claim dispute form must be completed in its. See coverage in your area;