Aetna Complaint And Appeal Form
Aetna Complaint And Appeal Form - Web this form is for your representative's use in making suggestions or filing formal complaints or appeals regarding any aspect of the aetna health plan or any physician, hospital, or other health care professional or health services organization providing your care as an enrollee/member of aetna. Address, phone number and practice changes behavioral health precertification coordination of benefits (cob) employee assistance program (eap) medicaid disputes and appeals medical precertification medicare disputes and appeals Web 3 ways to file a complaint you have the right to make your voice heard about your health care experience — whether it’s about us, your plan, a health service or provider. Or use our national fax number: (this information may be found on the front of the member’s id card.) today’s date member’s id number plan type member’s group number (optional) medical dental member’s first name member’s last. Web requiring submission of the aetna provider complaint and appeal form for all provider written complaints and all appeals. Web find all the forms you need find forms and applications for health care professionals and patients, all in one place. Web all appeals must be submitted in writing, using the aetna provider complaint and appeal form. Completion of this form is voluntary. These changes do not affect member appeals.
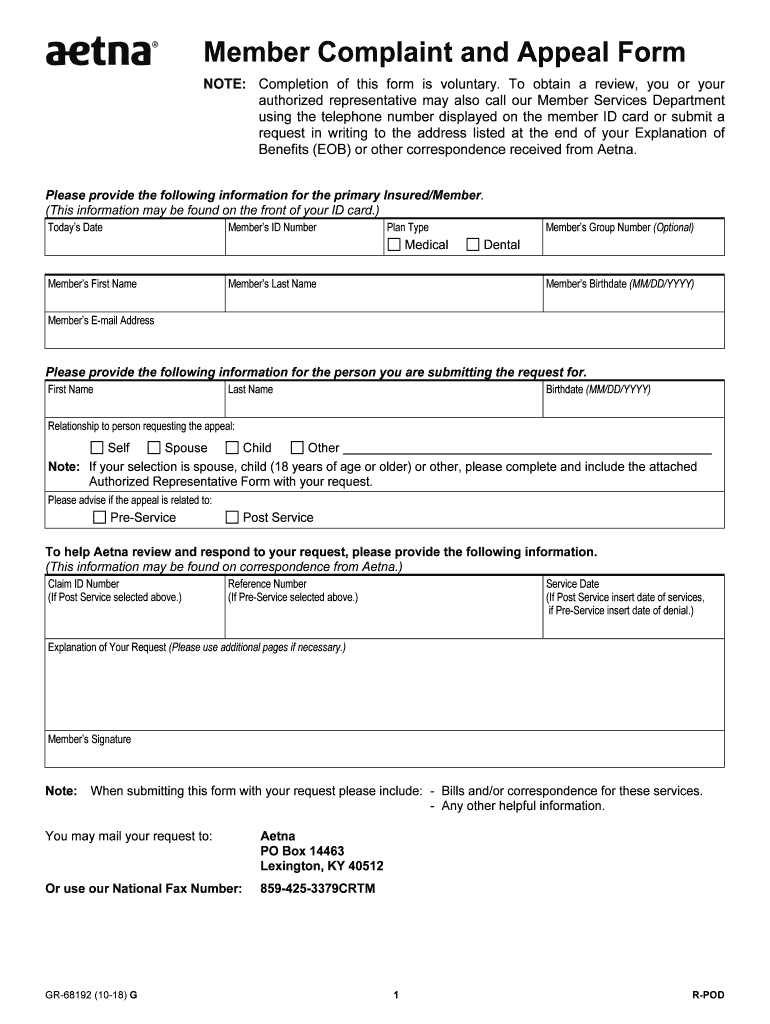
This requires all appeals to be submitted in writing. Web find all the forms you need find forms and applications for health care professionals and patients, all in one place. Web member complaint and appeal form. We’re here to make filing a complaint a little easier. To obtain a review, you’ll need to include this form along with the completed waiver of liability form. Web 3 ways to file a complaint you have the right to make your voice heard about your health care experience — whether it’s about us, your plan, a health service or provider. Completion of this form is voluntary. To obtain a review, you or your authorized representative may also call our member services department using the telephone number displayed on the member id card or submit a request in writing to the address listed at the end of your explanation of benefits (eob) or. Get a provider complaint and appeal form (pdf) Web please provide the following information.
Web complaint and appeal form. We’re here to make filing a complaint a little easier. Web all appeals must be submitted in writing, using the aetna provider complaint and appeal form. Get a provider complaint and appeal form (pdf) Web please provide the following information. (this information may be found on the front of the member’s id card.) today’s date member’s id number plan type member’s group number (optional) medical dental member’s first name member’s last. To obtain a review, you or your authorized representative may also call our member services department using the telephone number displayed on the member id card or submit a request in writing to the address listed at the end of your explanation of benefits (eob) or. Web 3 ways to file a complaint you have the right to make your voice heard about your health care experience — whether it’s about us, your plan, a health service or provider. Completion of this form is voluntary. Get a medicare provider complaint and appeal form (pdf) get a provider complaint and.
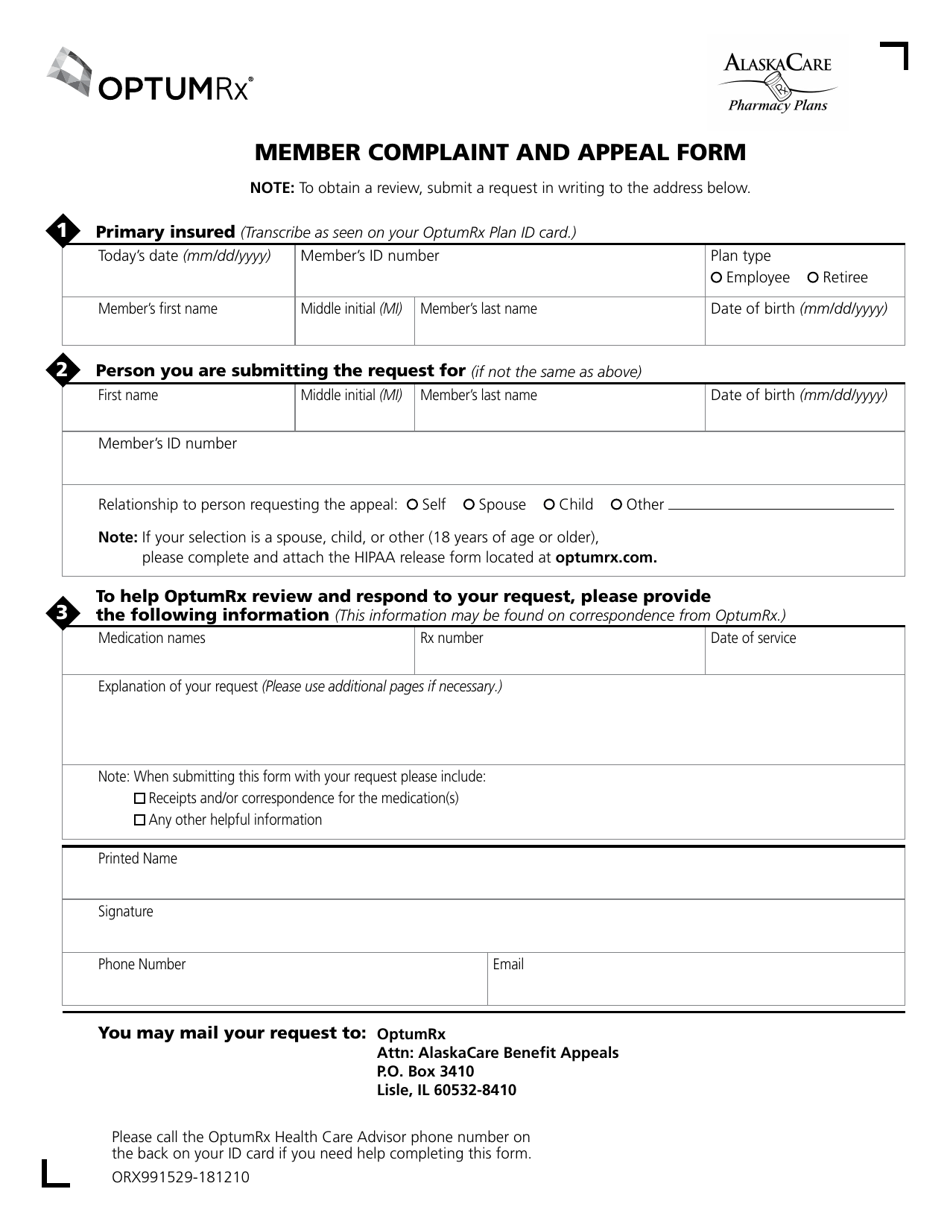
Alaska Member Complaint and Appeal Form Download Printable PDF
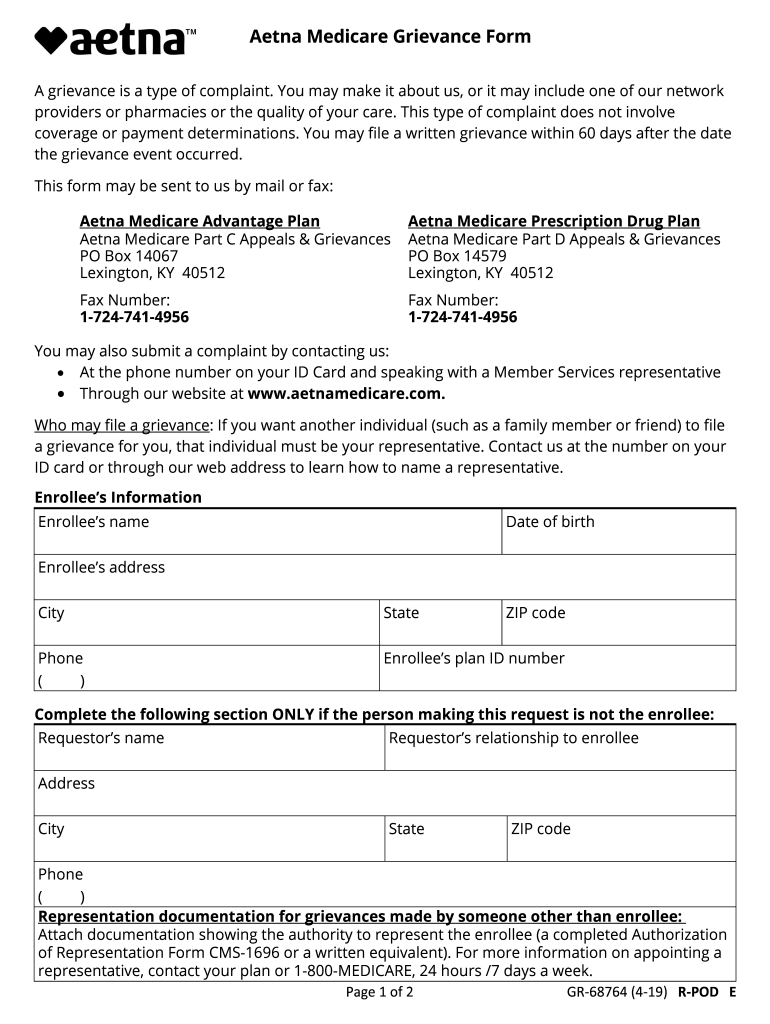
Get a medicare provider complaint and appeal form (pdf) get a provider complaint and. Web member complaint and appeal form. Or use our national fax number: Address, phone number and practice changes behavioral health precertification coordination of benefits (cob) employee assistance program (eap) medicaid disputes and appeals medical precertification medicare disputes and appeals Completion of this form is voluntary.

Aetna GR67902 2004 Fill and Sign Printable Template Online US
Make sure to include any information that will support your appeal. Or use our national fax number: Web member complaint and appeal form. Address, phone number and practice changes behavioral health precertification coordination of benefits (cob) employee assistance program (eap) medicaid disputes and appeals medical precertification medicare disputes and appeals Completion of this form is voluntary.
Medicare Part D Medication Prior Authorization Form Form Resume
Web 3 ways to file a complaint you have the right to make your voice heard about your health care experience — whether it’s about us, your plan, a health service or provider. (this information may be found on the front of the member’s id card.) today’s date member’s id number plan type member’s group number (optional) medical dental member’s.

Aetna Appeal Letter Sample Templates
This requires all appeals to be submitted in writing. Or use our national fax number: These changes do not affect member appeals. Completion of this form is voluntary. To obtain a review, you or your authorized representative may also call our member services department using the telephone number displayed on the member id card or submit a request in writing.
Member aetna com membersecure assets pdfs forms 68192 pdf Fill out
Web member complaint and appeal form. To obtain a review, you or your authorized representative may also call our member services department using the telephone number displayed on the member id card or submit a request in writing to the address listed at the end of your explanation of benefits (eob) or. You may mail your request to: Address, phone.

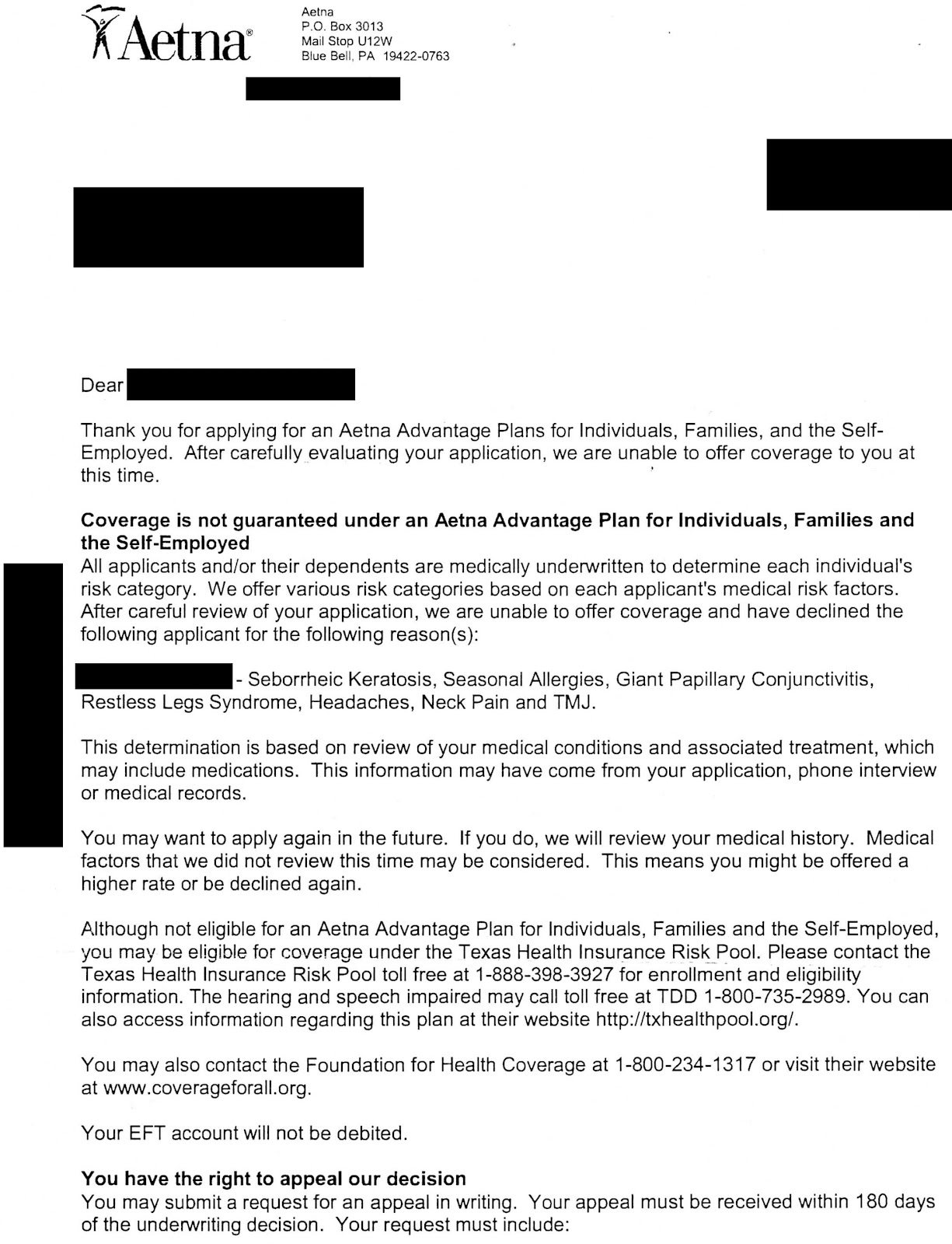
AETNA FAIL Here is the rejection letter from Aetna, my appeal, and the
Address, phone number and practice changes behavioral health precertification coordination of benefits (cob) employee assistance program (eap) medicaid disputes and appeals medical precertification medicare disputes and appeals Completion of this form is voluntary. Web requiring submission of the aetna provider complaint and appeal form for all provider written complaints and all appeals. To obtain a review, you or your authorized.
Aetna Medicare Complaint Team Fill Out and Sign Printable PDF
Web this form is for your representative's use in making suggestions or filing formal complaints or appeals regarding any aspect of the aetna health plan or any physician, hospital, or other health care professional or health services organization providing your care as an enrollee/member of aetna. Or use our national fax number: Web 3 ways to file a complaint you.

Aetna Appeal Letter Sample Templates
Web requiring submission of the aetna provider complaint and appeal form for all provider written complaints and all appeals. Web 3 ways to file a complaint you have the right to make your voice heard about your health care experience — whether it’s about us, your plan, a health service or provider. Make sure to include any information that will.
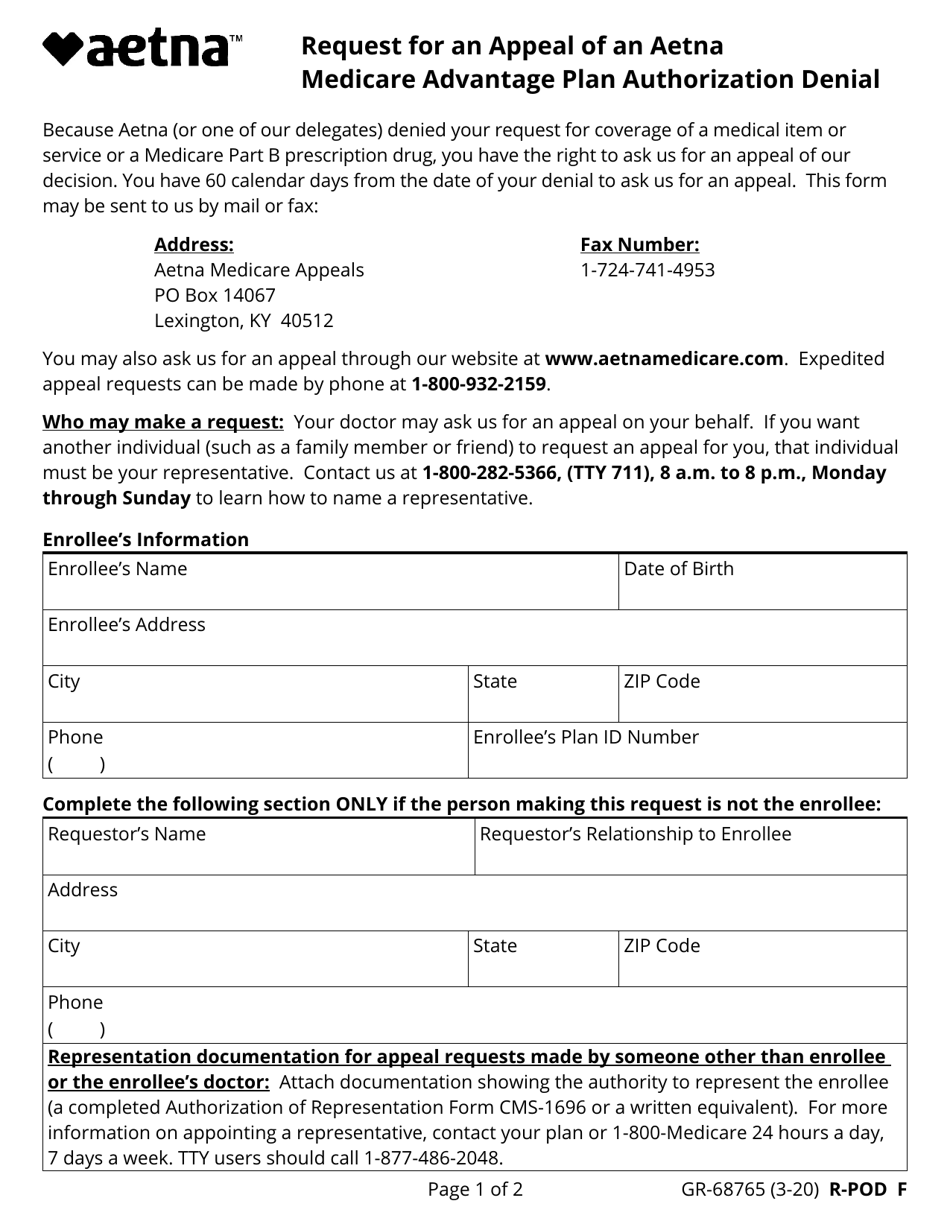
Form GR68765 Download Fillable PDF or Fill Online Request for an
Web requiring submission of the aetna provider complaint and appeal form for all provider written complaints and all appeals. Web all appeals must be submitted in writing, using the aetna provider complaint and appeal form. Address, phone number and practice changes behavioral health precertification coordination of benefits (cob) employee assistance program (eap) medicaid disputes and appeals medical precertification medicare disputes.
AETNA FAIL Here is the rejection letter from Aetna, my appeal, and the
You may mail your request to: These changes do not affect member appeals. Web please provide the following information. Address, phone number and practice changes behavioral health precertification coordination of benefits (cob) employee assistance program (eap) medicaid disputes and appeals medical precertification medicare disputes and appeals Web member complaint and appeal form.
Completion Of This Form Is Voluntary.
Web 3 ways to file a complaint you have the right to make your voice heard about your health care experience — whether it’s about us, your plan, a health service or provider. Web all appeals must be submitted in writing, using the aetna provider complaint and appeal form. Web this form is for your representative's use in making suggestions or filing formal complaints or appeals regarding any aspect of the aetna health plan or any physician, hospital, or other health care professional or health services organization providing your care as an enrollee/member of aetna. Web requiring submission of the aetna provider complaint and appeal form for all provider written complaints and all appeals.
Get A Provider Complaint And Appeal Form (Pdf)
Or use our national fax number: Web member complaint and appeal form. You may mail your request to: Web please provide the following information.
(This Information May Be Found On The Front Of The Member’s Id Card.) Today’s Date Member’s Id Number Plan Type Member’s Group Number (Optional) Medical Dental Member’s First Name Member’s Last.
Address, phone number and practice changes behavioral health precertification coordination of benefits (cob) employee assistance program (eap) medicaid disputes and appeals medical precertification medicare disputes and appeals Make sure to include any information that will support your appeal. This requires all appeals to be submitted in writing. Completion of this form is voluntary.
To Obtain A Review, You’ll Need To Include This Form Along With The Completed Waiver Of Liability Form.
Web member complaint and appeal form. To obtain a review, you or your authorized representative may also call our member services department using the telephone number displayed on the member id card or submit a request in writing to the address listed at the end of your explanation of benefits (eob) or. These changes do not affect member appeals. We’re here to make filing a complaint a little easier.